Hospital admittance and hospital observation are two distinct levels of care that patients may experience during a hospital stay, each with different implications for treatment, billing, and insurance coverage. Admittance typically involves a formal process where a patient is assigned an inpatient bed and receives intensive, round-the-clock care for a significant medical condition, often requiring complex treatments or surgeries. In contrast, observation status is a short-term arrangement where patients are monitored in a hospital setting for a limited period, usually 24 to 48 hours, to determine if they need inpatient admission or can be safely discharged. While both involve hospital care, admittance is billed as an inpatient stay, often covered by insurance with higher costs, whereas observation is billed as an outpatient service, which may result in higher out-of-pocket expenses for the patient depending on their insurance plan. Understanding the difference is crucial for patients to navigate potential financial and medical outcomes during their hospital visit.
Explore related products





What You'll Learn
![]()
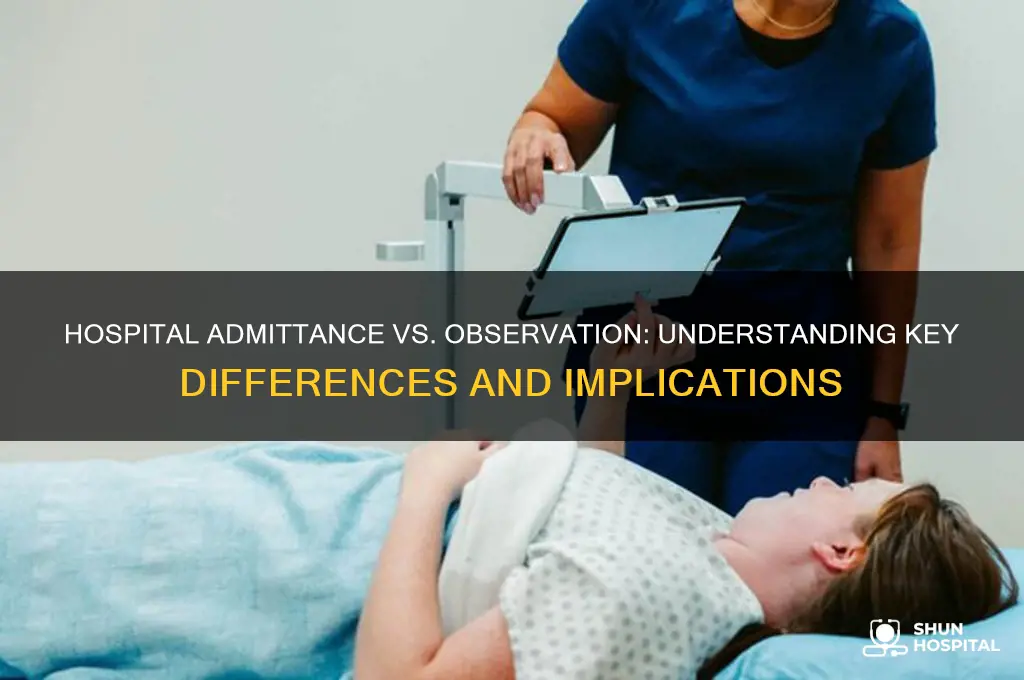
Admittance vs. Observation Status
Hospital admittance and observation status are two distinct classifications that significantly impact patient care, billing, and insurance coverage. Admittance occurs when a physician determines that a patient requires inpatient hospital care due to the severity or complexity of their condition. This status typically involves staying overnight in a hospital bed, receiving intensive treatments, and being under continuous medical supervision. In contrast, observation status is assigned when a patient’s condition is less clear-cut, and they are placed in a temporary holding pattern—often in an emergency department or dedicated observation unit—for monitoring, testing, or short-term treatment, usually lasting no more than 24 to 48 hours.
From a financial perspective, the difference between admittance and observation can be stark. Admitted patients are billed under Medicare Part A, which covers hospital stays and typically involves lower out-of-pocket costs for services like surgeries or specialist consultations. However, observation patients are billed under Medicare Part B, which treats their stay as an outpatient service, leading to higher copays and potential denial of coverage for subsequent skilled nursing facility care. For instance, a patient admitted for a heart attack might pay a flat deductible, while an observation patient with chest pain could face 20% coinsurance on all tests and treatments.
Clinically, the distinction affects the level of care provided. Admitted patients are prioritized for comprehensive interventions, such as IV medications, frequent vital sign checks, and consultations with specialists. Observation patients, while monitored closely, may receive limited interventions and are often discharged sooner if their condition stabilizes. For example, a 72-year-old with pneumonia might be admitted for IV antibiotics and oxygen therapy, whereas a 60-year-old with suspected pneumonia but stable vitals could be placed under observation for a chest X-ray and oral antibiotics.
Patients and caregivers must advocate for clarity regarding their status, as hospitals sometimes fail to communicate the implications. Asking direct questions like, “Am I admitted or under observation?” can prevent unexpected bills or gaps in care. Additionally, understanding the 2-Midnight Rule—a Medicare guideline suggesting that stays expected to last beyond two midnights should qualify for admittance—can help patients challenge observation status if it seems inappropriate. Proactive engagement ensures alignment between medical necessity and billing practices.
In summary, admittance and observation status differ in duration, intensity of care, billing mechanisms, and insurance implications. While admittance offers comprehensive inpatient treatment with lower costs, observation provides short-term monitoring at higher out-of-pocket expense. Recognizing these distinctions empowers patients to navigate the healthcare system more effectively, ensuring they receive appropriate care without financial surprises. Always verify your status and ask for documentation to protect your rights and resources.
Critical Access Hospitals: Filling the Rural Healthcare Gap
You may want to see also
Explore related products






![]()
Billing and Insurance Differences
Hospital admittance and observation status significantly impact billing and insurance coverage, often leaving patients with unexpected costs. Admitted patients are typically billed under inpatient services, which are covered at a higher rate by most insurance plans, including Medicare. However, observation status falls under outpatient services, meaning patients may face higher out-of-pocket costs for procedures, medications, and even hospital stays. For instance, a patient under observation might pay a 20% coinsurance for each service, while an admitted patient’s costs are often capped after meeting a deductible.
Consider a scenario where a 65-year-old Medicare beneficiary is hospitalized for chest pain. If admitted, Medicare Part A covers the stay, and the patient pays a fixed deductible. If placed under observation, Medicare Part B applies, requiring the patient to cover 20% of each service, plus separate charges for medications and tests. This distinction can result in thousands of dollars in additional costs, especially for prolonged stays. Always ask your healthcare provider about your status and its financial implications to avoid surprises.
Insurance companies often deny inpatient coverage for observation stays, even if the patient spends multiple days in the hospital. For example, a patient under observation for 48 hours might receive a bill for $5,000 in outpatient services, whereas an admitted patient’s equivalent stay could cost $1,500 after insurance. To mitigate this, review your insurance policy’s inpatient and outpatient coverage limits. Some plans require prior authorization for inpatient admissions, so ensure your provider communicates with your insurer to avoid denials.
A practical tip: Keep detailed records of your hospital stay, including the services provided and your status (admitted or observation). If billed incorrectly, dispute the charges with both the hospital and your insurer. For Medicare beneficiaries, the NOTICE Act requires hospitals to notify patients of their observation status within 36 hours, providing an opportunity to clarify billing expectations. Understanding these nuances can save you from financial strain and ensure you receive the coverage you’re entitled to.
Expressing Gratitude: How to Thank Your Host for Dinner and Hospitality
You may want to see also
Explore related products

![CPC Exam Prep + Medical Billing & Coding + Medical Terminology [3-IN-1]: The Unfair Advantage Career System: Pass the Exam & Get Hired | Exam Simulator, ATS Resume & Interview Kit + Custom AI Coach](https://m.media-amazon.com/images/I/61rrA2UQUaL._AC_UL320_.jpg)



![]()
Length of Stay Criteria
Hospital admittance and observation status differ significantly in how they handle patient care, and one of the most critical distinctions lies in the length of stay criteria. Admittance typically requires a patient to stay overnight or longer, often for complex treatments or surgeries, while observation status limits the stay to 24 to 48 hours for monitoring and assessment. This difference directly impacts billing, insurance coverage, and the level of care provided. For instance, Medicare Part A covers inpatient stays but may not cover observation services, leaving patients with unexpected out-of-pocket costs. Understanding these criteria is essential for both patients and healthcare providers to navigate the financial and clinical implications effectively.
From a comparative perspective, length of stay criteria serve as a dividing line between the two statuses. Inpatient admittance is reserved for cases where a patient’s condition requires intensive intervention, such as post-surgical recovery or severe illness. Observation status, on the other hand, is for patients whose conditions are less critical but still require close monitoring, like chest pain or dehydration. For example, a patient admitted for a heart attack might stay for 3 to 5 days, while someone under observation for suspected appendicitis might be discharged within 24 hours if surgery is deemed unnecessary. These criteria ensure resources are allocated appropriately, but they also highlight the need for clear communication to avoid patient confusion.
Practically speaking, patients should ask their healthcare provider about their status upon arrival at the hospital. If placed under observation, inquire about the expected duration and criteria for transitioning to inpatient admittance if needed. For instance, a patient with fluctuating vital signs might start in observation but be admitted if their condition worsens. Additionally, understanding the financial implications is crucial. Observation stays are often billed under Medicare Part B, which covers outpatient services but may require higher copays. Patients should also verify their insurance coverage for both statuses to avoid unexpected bills.
Analytically, the length of stay criteria reflect broader healthcare system priorities, balancing patient needs with resource management. Hospitals must adhere to these criteria to comply with insurance regulations and avoid penalties for overutilization. However, this can sometimes lead to challenges, such as patients being kept in observation longer than necessary to avoid inpatient costs or being discharged prematurely due to financial constraints. For example, a study found that 9.6% of observation stays exceeded 48 hours, often due to diagnostic delays or lack of available beds. This underscores the need for flexibility in criteria to prioritize patient outcomes over administrative guidelines.
In conclusion, length of stay criteria are a pivotal aspect of distinguishing hospital admittance from observation. They dictate not only the duration of care but also its financial and clinical implications. Patients should proactively seek clarity on their status and its consequences, while healthcare providers must balance adherence to criteria with individualized patient needs. By understanding these nuances, both parties can navigate the complexities of hospital care more effectively, ensuring appropriate treatment and minimizing financial surprises.
Hartford Hospital Heliport: The Building It's Perched On Top Of
You may want to see also
Explore related products






![]()
Patient Rights and Care Levels
Hospital admittance and observation status significantly impact patient rights and care levels, often in ways patients may not immediately recognize. Admitted patients are formally considered inpatients, granting them access to comprehensive hospital services, including specialized care, surgeries, and longer-term treatments. Observed patients, however, are classified as outpatients, limiting their access to certain services and often resulting in shorter monitoring periods. This distinction directly affects the scope of care a patient receives, with admitted patients typically receiving more intensive and prolonged treatment compared to those under observation.
Understanding these differences is crucial for patients to advocate for their rights effectively. For instance, Medicare beneficiaries must know that observation status can lead to higher out-of-pocket costs for services like skilled nursing facility care, which requires a three-day inpatient stay. Patients under observation may also face limitations in accessing certain medications or therapies that are only approved for inpatients. To navigate this, patients should proactively ask their healthcare providers about their status and its implications, ensuring they are fully informed about their care plan and financial responsibilities.
From a care perspective, the level of monitoring and intervention differs markedly between admittance and observation. Admitted patients are often placed in dedicated hospital rooms, with continuous access to nursing staff and medical equipment. Observed patients, on the other hand, may be in emergency departments or designated observation units, where monitoring is frequent but not as constant. For example, an admitted patient with pneumonia might receive intravenous antibiotics and oxygen therapy, while an observed patient with similar symptoms may only receive oral antibiotics and periodic vital sign checks.
Practical tips for patients include keeping a record of all communications with healthcare providers, including discussions about their status. Patients should also inquire about the criteria for transitioning from observation to admittance, especially if their condition worsens. For older adults or those with chronic conditions, understanding these distinctions can prevent unexpected financial burdens and ensure appropriate care. For instance, a 70-year-old patient with diabetes and chest pain should clarify their status to avoid complications in post-hospital care coverage.
In conclusion, patient rights and care levels are intrinsically tied to whether a patient is admitted or observed. By staying informed and actively engaging with healthcare providers, patients can ensure they receive the appropriate level of care and protect themselves from unforeseen consequences. This knowledge empowers individuals to make informed decisions, fostering a more transparent and effective healthcare experience.
Accessing Care at Sharpe Hospital in Weston, WV: A Step-by-Step Guide
You may want to see also
Explore related products





![]()
Impact on Medicare Coverage
Medicare beneficiaries often face significant financial and logistical challenges when their hospital stay is classified as "observation" rather than "admittance." This distinction, seemingly minor, can dramatically alter coverage for subsequent care, particularly skilled nursing facility (SNF) stays. Medicare Part A covers SNF care only if the patient has been formally admitted to the hospital for three consecutive days (not counting the discharge date). Observation status, however, does not count toward this requirement, leaving patients responsible for potentially exorbitant out-of-pocket costs. For instance, a 72-year-old with hip surgery placed under observation for 48 hours would need to pay the full cost of SNF rehabilitation, which averages $340 per day, as their observation time does not qualify them for Medicare coverage.
To mitigate this, beneficiaries should proactively inquire about their status upon hospital arrival and request admittance if their condition warrants it. Hospitals often prioritize observation status to avoid penalties under Medicare’s readmission reduction program, but patients have the right to advocate for their classification. Documentation is key: ask for written confirmation of your status daily, as hospitals may switch between observation and inpatient care without notification. If denied admittance, appeal the decision through Medicare’s expedited review process, which allows for a reconsideration within 72 hours.
The financial implications extend beyond SNF coverage. Observation status also affects Medicare Part B cost-sharing, where patients pay 20% of outpatient services, including expensive tests and medications. For example, a patient under observation receiving an MRI (average cost $2,600) would owe $520, whereas an admitted inpatient pays a flat deductible. Additionally, observation stays do not reset the Part B deductible, meaning multiple visits could compound costs. Beneficiaries should scrutinize their Explanation of Benefits (EOB) statements to identify observation charges and dispute inaccuracies.
Legislative efforts, such as the *Improving Access to Medicare Coverage Act*, aim to address these disparities by counting observation hours toward the three-day requirement. Until such reforms pass, patients must navigate the system vigilantly. Practical tips include electing Medicare Advantage plans, which sometimes offer SNF coverage without the three-day rule, or purchasing supplemental Medigap policies to offset Part B expenses. Ultimately, understanding the admittance-observation divide is crucial for Medicare beneficiaries to avoid unforeseen financial burdens and ensure access to necessary post-hospital care.
Urgent Care vs Hospital: What's the Difference?
You may want to see also
Frequently asked questions
Hospital admittance involves being formally admitted as an inpatient, typically requiring a stay in a hospital room, while hospital observation is a short-term status where patients are monitored in a designated area to determine if they need inpatient admission.
Yes, insurance often covers hospital admittance under inpatient benefits, which may have higher costs but more comprehensive coverage. Observation is typically billed as outpatient care, which may result in higher out-of-pocket costs for the patient.
Hospital observation is usually limited to 24 to 48 hours, though it can occasionally extend longer if necessary to determine the need for inpatient admission.
No, time spent under hospital observation does not count toward Medicare’s 3-day inpatient stay requirement for skilled nursing facility coverage, as observation is considered outpatient care.
While patients can express their preferences, the decision to admit or observe is made by the healthcare provider based on medical necessity. Patients should discuss their concerns with their doctor.































