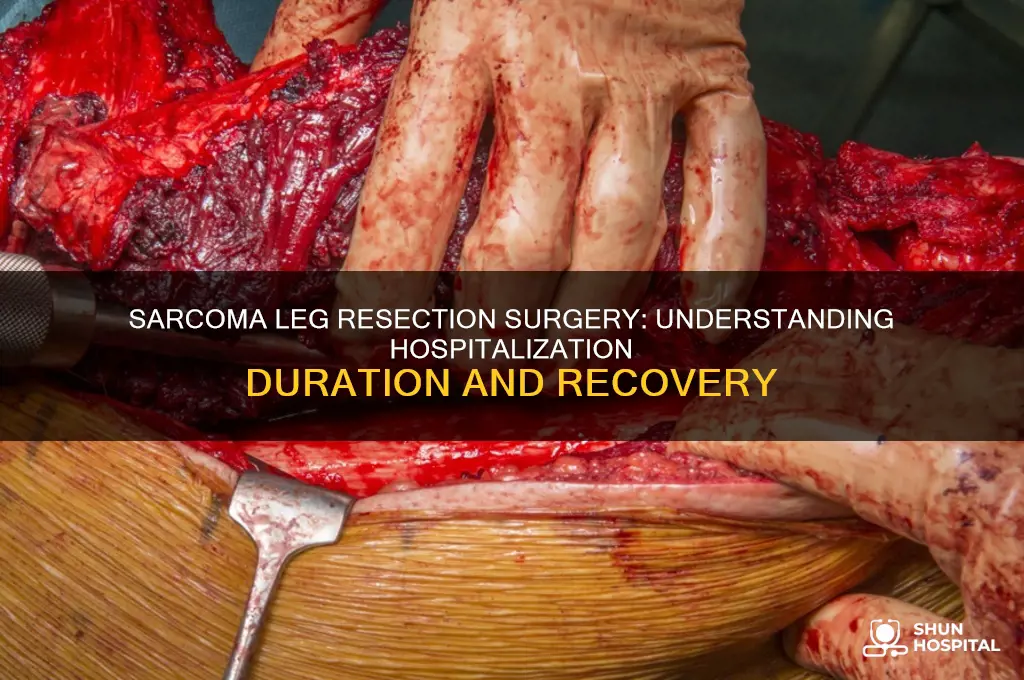
Sarcoma leg resection surgery is a complex procedure performed to remove cancerous tumors from the leg, often requiring careful planning and execution to ensure complete tumor removal while preserving limb function. Following the surgery, the hospitalization time can vary significantly depending on several factors, including the patient’s overall health, the extent of the resection, and any complications that may arise. On average, patients can expect to stay in the hospital for 3 to 7 days, during which time they will be closely monitored for signs of infection, bleeding, or other postoperative issues. Pain management, physical therapy, and wound care are also critical components of the recovery process during this period. In some cases, additional procedures or complications may extend the hospital stay, while healthier patients with straightforward recoveries may be discharged sooner. Ultimately, the healthcare team will determine the appropriate length of hospitalization based on individual patient needs and recovery progress.
Explore related products






What You'll Learn
- Pre-surgery preparation and planning for sarcoma leg resection hospitalization
- Average hospital stay duration after sarcoma leg resection surgery
- Factors influencing prolonged hospitalization post-sarcoma leg resection
- Post-surgery recovery and monitoring during hospital stay for sarcoma
- Discharge criteria and transition to home care after sarcoma resection
![]()
Pre-surgery preparation and planning for sarcoma leg resection hospitalization
The complexity of sarcoma leg resection surgery demands meticulous pre-surgery preparation to optimize outcomes and minimize hospitalization time. This phase is not merely administrative; it’s a critical window for patient education, risk mitigation, and logistical coordination. Patients typically undergo a series of diagnostic tests, including advanced imaging (MRI, CT scans) and biopsies, to delineate tumor size, location, and involvement of surrounding tissues. Surgeons and oncologists collaborate to devise a tailored surgical plan, often integrating input from physical therapists and prosthetists if limb salvage or amputation is anticipated. This interdisciplinary approach ensures that every stakeholder—from the anesthesiologist to the post-op nursing team—is aligned on the patient’s unique needs.
Pre-surgery preparation also involves rigorous patient optimization to reduce surgical risks. For instance, patients with comorbidities like diabetes or cardiovascular disease may require medication adjustments or lifestyle modifications weeks before surgery. Smoking cessation is strongly encouraged, as nicotine impairs wound healing and increases infection risk. Nutritional assessments are common, with supplements (e.g., vitamin D, iron) prescribed to address deficiencies. Patients are often advised to begin gentle lower-body strengthening exercises, under professional guidance, to enhance post-operative recovery. For example, simple ankle pumps or seated leg lifts can improve circulation and muscle tone without exacerbating the tumor site.
Logistical planning is another cornerstone of pre-surgery preparation. Patients and caregivers should arrange for transportation, as driving is prohibited for several weeks post-surgery. Home modifications—such as installing grab bars, removing trip hazards, and ensuring the surgical leg can be elevated—are essential for a safe recovery environment. Hospitals typically provide a pre-admission checklist, including fasting guidelines (usually 8–12 hours before surgery) and instructions on which medications to pause or continue. For instance, blood thinners like warfarin are often discontinued 3–5 days prior, under medical supervision, to minimize bleeding risks.
Psychological preparation is equally vital, as the emotional toll of sarcoma surgery can be profound. Hospitals may offer counseling sessions or support groups to help patients process anxiety and set realistic expectations. Caregivers are encouraged to attend pre-surgery meetings to understand their role in post-operative care, such as wound dressing changes or administering prescribed medications (e.g., opioids for pain management, typically tapered over 2–4 weeks). Clear communication with the healthcare team about concerns or preferences ensures that the patient’s voice remains central to the care plan.
Finally, pre-surgery preparation includes a detailed discussion of potential complications and their management. Patients are educated about signs of infection (e.g., fever, redness, pus), blood clots (swelling, warmth in the calf), or wound dehiscence (separation of surgical edges). Hospitals often provide emergency contact information and a timeline for follow-up appointments, typically starting within 7–14 days post-discharge. By addressing these elements proactively, patients and providers can significantly influence the efficiency of hospitalization and the trajectory of recovery.
Optical Shop Services at Dallas VA Hospital: Location and Offerings
You may want to see also
Explore related products






![]()
Average hospital stay duration after sarcoma leg resection surgery
The average hospital stay after sarcoma leg resection surgery typically ranges from 5 to 14 days, depending on factors like the extent of the surgery, the patient’s overall health, and complications. For instance, a patient undergoing a distal femur resection with endoprosthetic reconstruction may require a longer stay due to the complexity of the procedure and the need for early physical therapy to prevent joint stiffness. In contrast, a less invasive compartmental resection might allow for a shorter hospitalization period.
Several variables influence the duration of the hospital stay. Age plays a significant role, with older patients often requiring additional monitoring and recovery time. Comorbidities such as diabetes or cardiovascular disease can also extend hospitalization, as these conditions may slow wound healing or increase infection risk. For example, a 65-year-old patient with diabetes might stay 10–12 days, while a healthy 40-year-old could be discharged in 5–7 days. Postoperative complications, such as wound dehiscence or deep vein thrombosis, are another critical factor that can prolong recovery.
Pain management strategies are pivotal in determining hospital discharge timing. Patients receiving multimodal analgesia, combining opioids with non-opioid medications like acetaminophen and NSAIDs, often experience better pain control and earlier mobility. This approach not only reduces hospital stays but also minimizes opioid-related side effects, such as nausea and constipation, which can delay recovery. For instance, a patient on a well-managed pain regimen might transition to oral medications within 48 hours, paving the way for earlier discharge.
Rehabilitation protocols also impact hospital stay duration. Early physical therapy, initiated within 24–48 hours post-surgery, is standard practice to prevent muscle atrophy and joint contractures. Patients who actively participate in therapy, such as gait training with assistive devices, often progress faster. Hospitals with dedicated orthopedic oncology teams may streamline this process, reducing stays to 7–10 days. Conversely, delayed rehabilitation or insufficient support can extend hospitalization by 3–5 days.
Finally, practical tips can help patients and caregivers prepare for discharge. Ensuring home accessibility, such as installing grab bars and removing trip hazards, is essential for safety. Arranging follow-up appointments with oncologists and physical therapists within 1–2 weeks post-discharge ensures continuity of care. Patients should also stock up on prescribed medications and wound care supplies before leaving the hospital. By proactively addressing these details, patients can transition smoothly from hospital to home, minimizing the risk of readmission.
Exploring Madera Hospital's Secrets in 'Through the Looking Glass
You may want to see also
Explore related products





![]()
Factors influencing prolonged hospitalization post-sarcoma leg resection
The average hospitalization time for sarcoma leg resection surgery typically ranges from 5 to 14 days, but several factors can significantly extend this duration. Understanding these variables is crucial for patients and healthcare providers to anticipate and manage post-operative care effectively. Here’s a detailed breakdown of the key factors influencing prolonged hospitalization.
Complexity of the Surgery and Tumor Characteristics: The extent of the resection directly impacts recovery time. High-grade sarcomas or tumors located near critical structures like nerves or blood vessels often require more intricate surgical techniques, increasing the risk of complications such as bleeding, infection, or nerve damage. For instance, a patient undergoing a wide local excision with vascular reconstruction may face a longer hospital stay compared to someone with a less invasive procedure. Tumor size also plays a role; larger sarcomas (>5 cm) frequently necessitate more extensive surgery and longer recovery periods.
Patient-Specific Factors: Age, overall health, and comorbidities are critical determinants of hospitalization duration. Elderly patients (over 65) or those with pre-existing conditions like diabetes, cardiovascular disease, or compromised immune systems often experience slower wound healing and increased susceptibility to infections. For example, a 70-year-old patient with poorly controlled diabetes might require additional days in the hospital to manage blood sugar levels and prevent wound complications. Similarly, patients with obesity may face challenges in mobility and wound care, prolonging their recovery.
Post-Operative Complications: Infections, such as surgical site infections or deep vein thrombosis (DVT), are common reasons for extended hospitalization. Prophylactic measures like antibiotic administration (e.g., cefazolin 2g IV pre-operatively) and anticoagulant therapy (e.g., enoxaparin 40mg daily) are standard, but their effectiveness varies. Delayed wound healing, often exacerbated by poor blood flow or radiation therapy, can also extend hospital stays. For instance, a patient who develops a wound dehiscence may require an additional 5–7 days of hospitalization for wound management and potential revision surgery.
Rehabilitation Needs: The level of functional recovery required post-surgery significantly influences hospital discharge timing. Patients undergoing major limb-sparing procedures or those requiring prosthetic fitting often need intensive physical therapy before transitioning to home or a rehabilitation facility. A patient with a distal femur resection, for example, might spend an extra week in the hospital working with a physical therapist to regain mobility and strength. Early involvement of a multidisciplinary team, including physiotherapists and occupational therapists, can streamline this process but may still extend the overall hospitalization period.
Social and Support Factors: Discharge planning is as critical as the surgery itself. Patients without adequate home support or those living in remote areas may face delays in discharge due to logistical challenges. For instance, arranging home health services or securing transportation for follow-up appointments can add days to the hospital stay. Additionally, patients requiring specialized equipment, such as wheelchairs or wound care supplies, may experience delays until these resources are available. Addressing these social determinants of health proactively can mitigate prolonged hospitalization but often requires coordination across multiple healthcare and community services.
By addressing these factors—surgical complexity, patient health, complications, rehabilitation needs, and social support—healthcare providers can better manage expectations and optimize post-operative care for sarcoma leg resection patients. Tailored interventions and early planning are essential to minimizing unnecessary hospital stays while ensuring safe and effective recovery.
Urgent Doctor Dispatch: Strategies for Hospitals to Rapidly Fill Critical Roles
You may want to see also
Explore related products






![]()
Post-surgery recovery and monitoring during hospital stay for sarcoma
The initial 24–48 hours post-sarcoma leg resection surgery are critical for stabilizing the patient and managing acute pain. During this period, patients are typically monitored in an intensive care unit (ICU) or a dedicated surgical recovery ward. Vital signs such as heart rate, blood pressure, and oxygen saturation are closely watched to detect any complications like bleeding or infection. Pain management is a priority, often involving a combination of intravenous opioids (e.g., morphine or fentanyl) and nerve blocks, such as a femoral nerve block, to minimize discomfort while reducing reliance on systemic analgesics. Early mobility, such as ankle pumps or gentle leg lifts, may be encouraged to prevent blood clots, though weight-bearing restrictions are strictly enforced based on the extent of the resection.
Once stabilized, patients transition to a general surgical ward, where the focus shifts to wound care and physical therapy. Surgical incisions are inspected daily for signs of infection, such as redness, swelling, or discharge. Dressings are changed as needed, and drains, if placed, are monitored for output volume and color. Physical therapists begin working with patients within 48–72 hours post-surgery, starting with range-of-motion exercises and gradually progressing to strength-building activities. For example, patients might practice transferring from bed to chair, standing with support, or using a walker for short distances. Occupational therapists may also assist in adapting daily activities to accommodate temporary mobility limitations.
Nutrition plays a pivotal role in recovery, as the body requires adequate protein and calories to heal tissues and combat surgical stress. Patients are typically started on a clear liquid diet and advanced to solid foods as tolerated. A dietitian may recommend supplements, such as whey protein or vitamin D, to support muscle repair and bone health, particularly in older adults or those with pre-existing malnutrition. Hydration is equally important, with intravenous fluids often continued until oral intake is sufficient. Patients are encouraged to consume small, frequent meals to avoid nausea and ensure consistent nutrient intake.
Throughout the hospital stay, psychological support is integrated into the recovery plan. Coping with the loss of a limb or significant tissue can trigger anxiety, depression, or grief. Psychologists or counselors may meet with patients to provide coping strategies, while peer support groups or visits from prosthetists can offer hope and practical insights into life post-surgery. Family members are often involved in these sessions to foster a supportive home environment upon discharge. The average hospitalization time for sarcoma leg resection surgery ranges from 5 to 14 days, depending on factors like the patient’s overall health, the complexity of the surgery, and the presence of complications.
Before discharge, a comprehensive plan is developed to ensure a smooth transition to home or a rehabilitation facility. Patients receive detailed instructions on wound care, medication management (e.g., oral pain relievers, blood thinners like aspirin or enoxaparin), and follow-up appointments with surgeons and oncologists. Physical therapy exercises are prescribed for home use, often with the assistance of a visiting therapist or caregiver. Warning signs of complications, such as fever, increased pain, or drainage from the incision, are emphasized, along with clear instructions on when to seek emergency care. This structured approach minimizes readmissions and maximizes long-term recovery outcomes.
Essential Pediatric Hospital Packing List: Comfort and Care for Kids
You may want to see also
Explore related products






![]()
Discharge criteria and transition to home care after sarcoma resection
The average hospitalization time for sarcoma leg resection surgery typically ranges from 5 to 10 days, depending on factors like the extent of the surgery, the patient’s overall health, and complications. However, the transition from hospital to home care is just as critical as the surgery itself. Discharge criteria are meticulously designed to ensure patient safety and recovery continuity. These criteria include stable vital signs, adequate pain management, and the ability to perform basic activities with assistance. For instance, patients must demonstrate proficiency in using mobility aids like crutches or walkers, as well as understanding wound care protocols. Without meeting these benchmarks, premature discharge could lead to complications such as infection or delayed healing.
Instructive guidance for the transition to home care begins with a detailed care plan provided by the healthcare team. Patients and caregivers should receive clear instructions on medication management, including dosages and schedules for pain relievers (e.g., opioids or NSAIDs) and antibiotics. For example, a typical post-surgery regimen might involve oxycodone 5 mg every 4–6 hours for pain, coupled with cefadroxil 500 mg twice daily for infection prevention. Physical therapy exercises, such as ankle pumps and gentle leg lifts, should be practiced daily to prevent stiffness and promote circulation. Caregivers must also be trained to monitor for signs of complications, such as fever, increased swelling, or drainage from the surgical site, and know when to seek medical attention.
Persuasively, the success of home care hinges on patient adherence to the prescribed plan and open communication with the healthcare team. Patients often underestimate the importance of follow-up appointments, which are crucial for monitoring healing progress and adjusting treatment as needed. For example, a 45-year-old patient who skips physical therapy sessions may experience muscle atrophy, prolonging recovery. Similarly, ignoring dietary recommendations—such as consuming adequate protein (1.2–1.5 g/kg/day) to support tissue repair—can hinder wound healing. By emphasizing these points, healthcare providers can empower patients to take an active role in their recovery.
Comparatively, the transition to home care after sarcoma resection differs significantly from other orthopedic surgeries due to the complexity of the procedure and the risk of cancer recurrence. Unlike a routine knee replacement, sarcoma patients may require additional precautions, such as avoiding excessive weight-bearing activities for 6–8 weeks to ensure proper bone and soft tissue healing. Moreover, the emotional toll of cancer treatment necessitates psychological support, which is often integrated into the home care plan. For instance, a 32-year-old patient might benefit from counseling sessions to address anxiety about recurrence, alongside physical rehabilitation.
Descriptively, the first few days at home can be challenging but manageable with proper preparation. Patients should arrange their living space to minimize obstacles and ensure easy access to essentials like medications, wound care supplies, and mobility aids. A raised toilet seat and shower chair can significantly ease daily activities. Meal preparation in advance, such as cooking nutrient-rich soups or casseroles, reduces the strain on the patient and caregiver. Additionally, establishing a routine—such as morning exercises followed by rest periods—provides structure and promotes healing. With these measures in place, the transition to home care becomes a manageable step toward full recovery.
Alan Jackson Hospitalized: What We Know So Far
You may want to see also
Frequently asked questions
The typical hospitalization time for sarcoma leg resection surgery ranges from 3 to 7 days, depending on the complexity of the surgery, the patient's overall health, and recovery progress.
Yes, hospitalization time can vary based on factors such as the extent of the resection, complications during or after surgery, and the need for additional procedures like reconstructive surgery or wound management.
Factors influencing hospital stay include the patient's age, overall health, the size and location of the tumor, the presence of complications (e.g., infection or bleeding), and the need for post-operative therapies like physical therapy or pain management.



















