Hospital-acquired infections (HAIs) pose a significant threat to patient safety, increasing morbidity, mortality, and healthcare costs. To combat this issue, a comprehensive plan solution must be implemented, focusing on multifaceted strategies. This includes stringent hand hygiene protocols for all healthcare personnel, rigorous environmental cleaning and disinfection practices, and the appropriate use of personal protective equipment (PPE). Additionally, implementing antimicrobial stewardship programs to optimize antibiotic use, isolating infected patients when necessary, and fostering a culture of safety through staff education and training are crucial components. By integrating these measures, hospitals can significantly reduce the incidence of HAIs, improve patient outcomes, and enhance overall healthcare quality.
Explore related products






What You'll Learn
- Hand Hygiene Protocols: Implement strict handwashing guidelines for all staff and visitors to reduce pathogen transmission
- Environmental Cleaning: Regularly disinfect high-touch surfaces and patient areas using standardized cleaning procedures
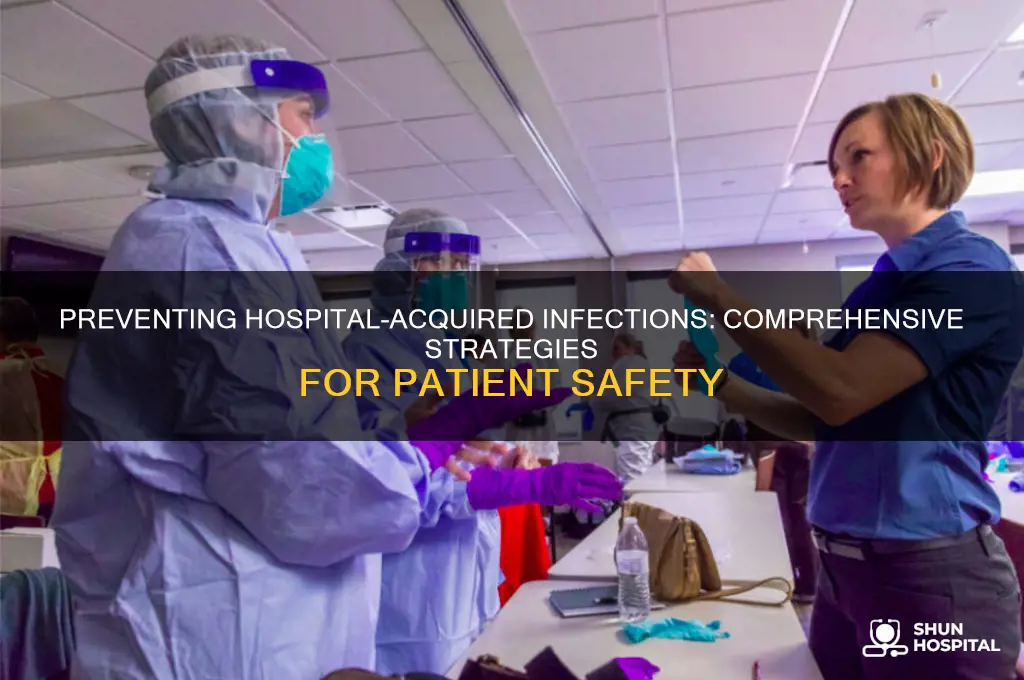
- Personal Protective Equipment (PPE): Ensure proper use of PPE, including gloves, masks, and gowns, for all healthcare workers
- Isolation Precautions: Isolate infected patients and follow contact, droplet, or airborne precautions to prevent spread
- Antibiotic Stewardship: Optimize antibiotic use to minimize resistance and reduce infection risks in patients
![]()
Hand Hygiene Protocols: Implement strict handwashing guidelines for all staff and visitors to reduce pathogen transmission
Hospital-acquired infections (HAIs) are a significant concern, contributing to prolonged hospital stays, increased healthcare costs, and, in severe cases, mortality. Among the myriad strategies to combat HAIs, hand hygiene stands out as one of the most effective and cost-efficient measures. The World Health Organization (WHO) estimates that proper hand hygiene can reduce HAI rates by up to 50%, underscoring its critical role in infection prevention. Despite its simplicity, adherence to hand hygiene protocols remains inconsistent across healthcare settings, necessitating stricter guidelines and enforcement.
Implementing strict handwashing guidelines begins with education. All staff, from physicians to custodial workers, and visitors must be trained on the *when* and *how* of hand hygiene. The WHO’s "Five Moments for Hand Hygiene" provides a clear framework: before touching a patient, before clean/aseptic procedures, after body fluid exposure risk, after touching a patient, and after touching patient surroundings. Training should emphasize the use of alcohol-based hand rubs (ABHR) with at least 60% alcohol for routine hand hygiene, as they are more effective and faster than soap and water unless hands are visibly soiled. For example, a 3–5 ml dose of ABHR, rubbed thoroughly for 20–30 seconds, ensures all surfaces of the hands are covered.
Enforcement of these protocols requires a multi-faceted approach. Hospitals should strategically place ABHR dispensers at point-of-care locations, ensuring accessibility within 3–5 steps of patient zones. Regular audits and feedback mechanisms, such as direct observation or electronic monitoring systems, can track compliance rates. Incentives for high compliance and constructive feedback for lapses can foster a culture of accountability. For instance, some hospitals have implemented "hand hygiene champions" who model best practices and provide peer-to-peer coaching, significantly improving adherence rates.
Visitors, often overlooked in hand hygiene initiatives, play a crucial role in pathogen transmission. Hospitals should mandate hand hygiene for visitors through clear signage, verbal reminders, and accessible sanitizing stations at entrances and patient rooms. A study in *Infection Control & Hospital Epidemiology* found that visitor compliance increased from 20% to 70% when combined with education and easy access to ABHR. Practical tips, such as placing dispensers at eye level and using colorful, multilingual signage, can enhance engagement.
While hand hygiene is a cornerstone of HAI prevention, it is not without challenges. Over-reliance on ABHR can lead to skin irritation, particularly among healthcare workers who perform hand hygiene dozens of times daily. Hospitals should provide moisturizing lotions and encourage their use after shifts to mitigate dryness. Additionally, addressing misconceptions, such as the belief that gloves eliminate the need for hand hygiene, is vital. Gloves can become contaminated during removal, emphasizing the need for hand hygiene immediately afterward.
In conclusion, strict hand hygiene protocols are a low-cost, high-impact solution to reducing HAIs. By combining education, accessibility, enforcement, and inclusivity of all hospital personnel and visitors, healthcare facilities can significantly lower infection rates. The key lies in consistent adherence, supported by a culture that prioritizes patient safety above all else. Hand hygiene is not just a protocol—it’s a lifeline.
Hospitals: Are Patient Satisfaction Scores Enough?
You may want to see also
Explore related products






![]()
Environmental Cleaning: Regularly disinfect high-touch surfaces and patient areas using standardized cleaning procedures
Hospital-acquired infections (HAIs) are a persistent challenge, with surfaces acting as silent reservoirs for pathogens. Environmental cleaning, specifically targeting high-touch surfaces, is a cornerstone of infection prevention. These surfaces—bed rails, doorknobs, light switches, and medical equipment—are frequently contaminated and serve as vectors for transmission. A single contaminated surface can harbor pathogens for days, putting patients, healthcare workers, and visitors at risk.
Standardized cleaning procedures are not just about wiping down surfaces; they are a systematic approach to ensure consistency and effectiveness. Protocols should specify the type of disinfectant, concentration (e.g., 1:10 bleach solution or EPA-approved hospital-grade disinfectants), contact time (typically 1–10 minutes), and frequency (e.g., twice daily in patient rooms, after each use for equipment). Audits and checklists can verify compliance, while color-coded microfiber cloths prevent cross-contamination between areas.
The human factor is critical. Staff training must emphasize the "why" behind cleaning protocols, not just the "how." Visual aids, such as glow germ simulations, can demonstrate the invisible spread of pathogens, reinforcing the importance of thorough cleaning. Additionally, feedback mechanisms, like real-time monitoring systems or patient-reported cleanliness scores, can hold teams accountable and drive continuous improvement.
Comparing manual cleaning to newer technologies highlights both strengths and limitations. While manual cleaning remains the gold standard for accessibility and cost-effectiveness, innovations like UV-C light disinfection and electrostatic sprayers offer supplemental benefits. However, these technologies should not replace manual cleaning but rather enhance it, particularly in hard-to-reach areas or during outbreak scenarios.
The takeaway is clear: environmental cleaning is not a one-size-fits-all task but a strategic, evidence-based practice. By standardizing procedures, investing in staff education, and integrating technology where appropriate, hospitals can significantly reduce the risk of HAIs. Clean surfaces are not just a matter of aesthetics—they are a lifeline in the fight against infection.
Mild Heart Attack Recovery: Typical Hospital Stay Duration Explained
You may want to see also
Explore related products






![]()
Personal Protective Equipment (PPE): Ensure proper use of PPE, including gloves, masks, and gowns, for all healthcare workers
Hospital-acquired infections (HAIs) are a significant concern, contributing to prolonged hospital stays, increased healthcare costs, and, in severe cases, mortality. One of the most effective strategies to mitigate this risk is the proper use of Personal Protective Equipment (PPE) by healthcare workers. Gloves, masks, and gowns act as critical barriers, preventing the transmission of pathogens between patients and healthcare providers. However, the effectiveness of PPE hinges not just on its availability but on its correct usage, which is often overlooked in high-pressure clinical environments.
Consider the donning and doffing of PPE, a process that requires precision and adherence to protocols. For instance, gloves should be worn when direct contact with blood, bodily fluids, or contaminated surfaces is anticipated. However, simply wearing gloves is insufficient; they must be changed between patients and tasks to avoid cross-contamination. Masks, particularly N95 respirators or surgical masks, must fit snugly to ensure filtration of airborne particles. A common mistake is touching the outer surface of the mask, which can transfer pathogens to the wearer’s hands. Gowns, whether disposable or reusable, should fully cover the torso and fit comfortably to prevent exposure during procedures. Training healthcare workers on these specifics is not optional—it’s a cornerstone of infection prevention.
The persuasive argument for PPE compliance lies in its proven impact. Studies show that proper PPE usage can reduce HAI rates by up to 70% in certain settings. For example, during the COVID-19 pandemic, hospitals that enforced strict PPE protocols saw significantly lower transmission rates among staff and patients. Yet, compliance remains a challenge. Fatigue, time constraints, and discomfort often lead to shortcuts. Addressing these barriers requires a multifaceted approach: providing high-quality, well-fitting PPE, ensuring accessibility, and fostering a culture of accountability. Leadership plays a pivotal role here; when administrators and senior staff model proper PPE use, it sets a standard for the entire team.
Comparatively, the cost of investing in PPE and training is minimal when weighed against the financial and human toll of HAIs. A single HAI can add $10,000 to $40,000 to a patient’s hospital bill, not to mention the emotional burden on families. In contrast, the expense of equipping a healthcare worker with gloves, masks, and gowns for a shift is negligible. Moreover, reusable PPE, such as washable gowns, offers a sustainable solution that reduces long-term costs while maintaining efficacy. Hospitals that adopt such practices not only protect their patients but also demonstrate fiscal responsibility.
In conclusion, ensuring proper PPE use is a non-negotiable element of HAI prevention. It requires a combination of education, accessibility, and accountability. By treating PPE protocols as a priority, healthcare facilities can create a safer environment for both patients and staff. The takeaway is clear: PPE is not just equipment—it’s a lifeline. Its proper use is a testament to a hospital’s commitment to patient safety and a critical step in the broader plan to eliminate HAIs.
Shingles Isolation in Hospitals: Necessary Precaution or Common Practice?
You may want to see also
Explore related products






![]()
Isolation Precautions: Isolate infected patients and follow contact, droplet, or airborne precautions to prevent spread
Hospital-acquired infections (HAIs) are a significant concern, contributing to prolonged hospital stays, increased healthcare costs, and, in severe cases, mortality. One of the most effective strategies to mitigate this risk is the implementation of isolation precautions, which involve separating infected patients and adhering to specific protocols based on the mode of transmission—contact, droplet, or airborne. This approach not only protects other patients but also safeguards healthcare workers and visitors from potential exposure.
Step-by-Step Implementation: To effectively isolate infected patients, hospitals must first identify the type of infection and its transmission route. For contact precautions, which apply to infections spread by direct or indirect contact (e.g., MRSA, C. difficile), patients should be placed in private rooms or cohorted with others having the same infection. Healthcare providers must wear gloves and gowns for all interactions and ensure that shared equipment is thoroughly disinfected. For droplet precautions (e.g., influenza, bacterial meningitis), patients should be masked and placed in private rooms or areas with at least 3 feet of separation from others. Healthcare workers should wear surgical masks when within this range. Airborne precautions (e.g., tuberculosis, measles) require negative-pressure rooms with at least 6 to 12 air changes per hour and the use of N95 respirators by staff.
Practical Tips for Success: Consistency is key. Staff training should emphasize the importance of adhering to these protocols, even in high-pressure situations. Visual aids, such as signage indicating the type of isolation required, can serve as reminders. Additionally, hospitals should maintain adequate supplies of personal protective equipment (PPE) and ensure its proper use through regular audits. For pediatric patients, age-appropriate explanations and distractions can help reduce anxiety during isolation.
Comparative Analysis: While isolation precautions are resource-intensive, their cost-effectiveness is evident when compared to the financial and human toll of untreated HAIs. For instance, a study in *The Lancet* found that proper isolation practices reduced HAI rates by up to 70% in intensive care units. However, challenges such as limited room availability and staff fatigue must be addressed through strategic planning and workforce management.
Takeaway: Isolation precautions are a cornerstone of infection control, requiring meticulous planning and execution. By tailoring protocols to the specific needs of each infection type, hospitals can significantly reduce the spread of HAIs. This not only improves patient outcomes but also reinforces public trust in healthcare systems. As healthcare evolves, continuous evaluation and adaptation of these practices will remain essential.
Exploring Halifax Hospital: Key Departments and Facilities Overview
You may want to see also
Explore related products





![Graduated Emesis Basins 700ML [Pack of 5] Graduated Kidney Shaped Bowl – Sturdy Plastic Irrigation Basin Tray](https://m.media-amazon.com/images/I/61D1kxKVM8L._AC_UL320_.jpg)
![]()
Antibiotic Stewardship: Optimize antibiotic use to minimize resistance and reduce infection risks in patients
Antibiotic stewardship is a critical strategy in the fight against hospital-acquired infections (HAIs), aiming to optimize antibiotic use to minimize resistance and protect patients. Overprescribing and misuse of antibiotics have accelerated the emergence of drug-resistant bacteria, making infections harder to treat. By implementing structured stewardship programs, hospitals can ensure that the right antibiotic is used at the right dose, for the right duration, and only when necessary. This approach not only preserves the efficacy of existing antibiotics but also reduces the risk of HAIs by minimizing disruptions to patients’ natural microbiomes.
Consider the following steps to establish an effective antibiotic stewardship program. First, designate a multidisciplinary team, including infectious disease specialists, pharmacists, and clinicians, to oversee antibiotic prescribing practices. This team should develop and enforce evidence-based guidelines tailored to the hospital’s patient population. For example, in pediatric patients, antibiotics like amoxicillin should be dosed at 50 mg/kg/day for mild infections, while adults with severe infections may require higher doses of broad-spectrum antibiotics like piperacillin-tazobactam (4.5 g every 6 hours). Second, implement a prior authorization process for restricted antibiotics, ensuring their use is justified. Third, regularly audit prescribing patterns and provide feedback to clinicians to promote adherence to guidelines.
A key challenge in antibiotic stewardship is balancing the need to treat infections promptly with the risk of overuse. For instance, empiric therapy—starting antibiotics before confirming an infection—is often necessary in critically ill patients but can contribute to resistance if not de-escalated once culture results are available. Hospitals should adopt protocols for de-escalation, such as switching from broad-spectrum to narrow-spectrum antibiotics within 48 hours of initiating therapy. Additionally, procalcitonin testing can help differentiate bacterial from viral infections, reducing unnecessary antibiotic use. For example, in patients with respiratory infections, a procalcitonin level below 0.1 ng/mL suggests a viral etiology, making antibiotics unwarranted.
The benefits of antibiotic stewardship extend beyond reducing resistance. By minimizing antibiotic exposure, patients are less likely to develop *Clostridioides difficile* infections (CDIs), a common HAI linked to antibiotic disruption of gut flora. Hospitals can further mitigate CDI risk by restricting high-risk antibiotics like clindamycin and fluoroquinolones, which are strongly associated with CDI. Practical tips for clinicians include emphasizing hand hygiene, isolating CDI patients, and educating patients about the risks of unnecessary antibiotics. For example, a 70-year-old patient on a prolonged course of ceftriaxone for a urinary tract infection should be monitored for CDI symptoms, such as diarrhea, and tested promptly if symptoms arise.
In conclusion, antibiotic stewardship is a multifaceted solution to prevent HAIs by optimizing antibiotic use. By combining structured protocols, multidisciplinary collaboration, and evidence-based practices, hospitals can reduce resistance, minimize infection risks, and improve patient outcomes. Success requires ongoing commitment, regular evaluation, and adaptation to emerging challenges, ensuring that antibiotics remain effective for future generations.
Steps to Become a Hospital Interpreter in Oregon
You may want to see also
Frequently asked questions
The primary plan involves implementing a multifaceted approach, including hand hygiene, infection surveillance, proper use of personal protective equipment (PPE), environmental cleaning, and antibiotic stewardship programs.
Hand hygiene is critical as it breaks the chain of infection by removing pathogens from healthcare workers' hands. Adherence to WHO’s "Five Moments for Hand Hygiene" significantly reduces the risk of transmitting infections.
Environmental cleaning ensures that surfaces and equipment in healthcare settings are free from pathogens. Regular disinfection of high-touch areas, such as bed rails and doorknobs, minimizes the risk of cross-contamination.
Antibiotic stewardship promotes the appropriate use of antibiotics, reducing the overuse and misuse that can lead to antibiotic resistance. This helps prevent infections caused by multidrug-resistant organisms.
Patient isolation, such as contact, droplet, or airborne precautions, prevents the spread of infectious agents by separating infected patients from others. This limits exposure and reduces the transmission of pathogens within the hospital.





![Dimes Peri Bottle for Postpartum Care [3-Pack] – 8 oz Perineal Squirt Bottle – Postpartum Essentials for New Moms – Easy to use Portable Bidet for women](https://m.media-amazon.com/images/I/619vI00JL8L._AC_UL320_.jpg)

























