Hospital-acquired infections (HAIs), also known as nosocomial infections, are a significant public health concern, affecting millions of patients worldwide each year. Quantitative data on HAIs is essential for understanding their prevalence, impact, and trends, enabling healthcare providers and policymakers to implement effective prevention and control measures. This data typically includes infection rates, such as central line-associated bloodstream infections (CLABSIs), catheter-associated urinary tract infections (CAUTIs), surgical site infections (SSIs), and ventilator-associated pneumonia (VAP), often measured per 1,000 patient-days or per 100 procedures. Additionally, metrics like patient mortality, length of hospital stay, and associated healthcare costs are analyzed to assess the burden of HAIs. Surveillance systems, such as the National Healthcare Safety Network (NHSN) in the United States, play a crucial role in collecting and reporting this data, facilitating benchmarking and evidence-based interventions to reduce infection rates and improve patient safety.
Explore related products






What You'll Learn
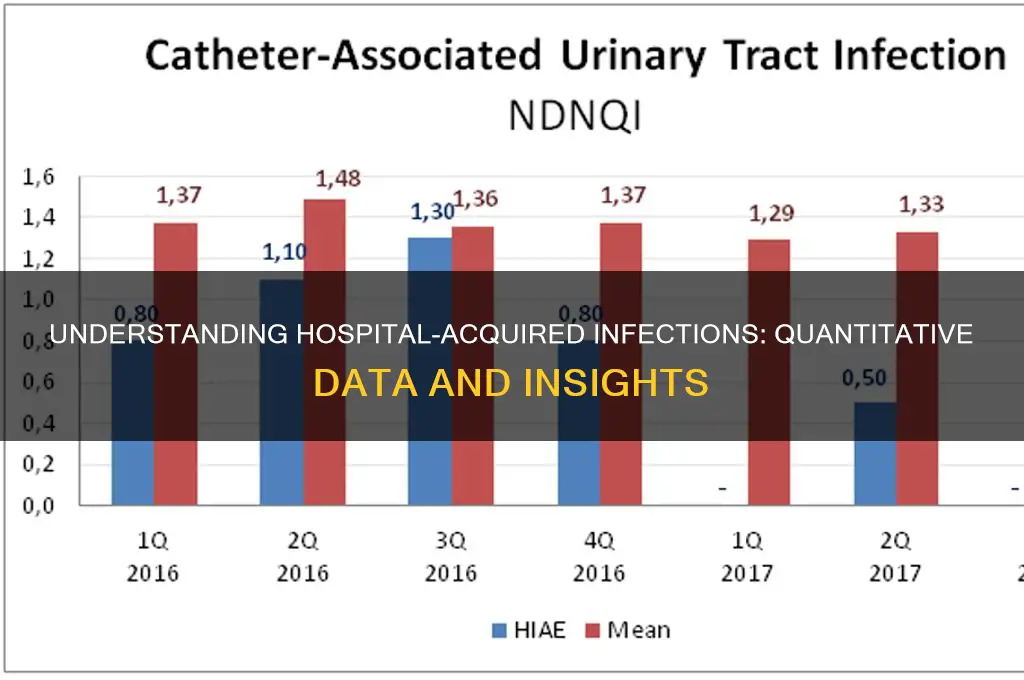
- Incidence Rates: Number of HAIs per 1,000 patient-days, stratified by infection type and unit
- Prevalence Data: Percentage of patients with HAIs at a specific point in time
- Mortality Statistics: HAI-related death rates and their impact on patient outcomes
- Cost Analysis: Financial burden of HAIs on healthcare systems, including treatment and extended stays
- Trends Over Time: Yearly or quarterly changes in HAI rates and prevention effectiveness
![]()
Incidence Rates: Number of HAIs per 1,000 patient-days, stratified by infection type and unit
Hospital-acquired infections (HAIs) are a critical metric in healthcare, and incidence rates—measured as the number of HAIs per 1,000 patient-days—offer a standardized way to compare infection burdens across units and facilities. This metric accounts for variations in patient volume and length of stay, providing a more accurate reflection of infection control effectiveness. For instance, a surgical intensive care unit (SICU) might report 5.2 central line-associated bloodstream infections (CLABSIs) per 1,000 patient-days, while a medical-surgical unit reports 2.8 catheter-associated urinary tract infections (CAUTIs) per 1,000 patient-days. These figures highlight disparities in infection types and unit-specific risks, guiding targeted interventions.
Stratifying incidence rates by infection type reveals patterns that inform prevention strategies. CLABSIs, CAUTIs, surgical site infections (SSIs), and ventilator-associated events (VAEs) are among the most tracked HAIs. For example, SSIs are more prevalent in orthopedic units due to the nature of invasive procedures, while CAUTIs are common in long-term care settings where catheter use is frequent. Analyzing these trends helps identify high-risk areas. A unit with a VAE rate of 3.5 per 1,000 patient-days may need to focus on ventilator bundle compliance, whereas a unit with a high SSI rate might benefit from enhanced sterile technique training.
Practical implementation of incidence rate data requires careful interpretation and action. Start by benchmarking your unit’s rates against national averages or peer institutions. For instance, the CDC’s National Healthcare Safety Network (NHSN) provides standardized infection ratios (SIRs) for comparison. If your SICU’s CLABSI rate exceeds the national SIR of 1.0, investigate contributing factors such as hand hygiene compliance, central line insertion practices, and dressing changes. Next, tailor interventions to the specific infection type and unit dynamics. For example, a CAUTI reduction program might include catheter insertion training, reminders to remove unnecessary catheters, and patient education on alternatives.
Cautions must be taken when using incidence rates to avoid misinterpretation. A low patient-day denominator can skew results, making small outbreaks appear more significant. For example, a small neonatal unit with 1 VAE in 500 patient-days would report a rate of 2.0, which might seem high but reflects limited data. Additionally, patient populations vary in susceptibility; a unit treating immunocompromised patients may have higher HAI rates despite optimal care. Always consider clinical context and adjust strategies accordingly. Regularly review data trends rather than relying on isolated incidents to ensure meaningful improvements.
In conclusion, incidence rates per 1,000 patient-days are a powerful tool for monitoring and reducing HAIs, but their utility depends on thoughtful analysis and action. By stratifying data by infection type and unit, healthcare providers can pinpoint vulnerabilities and implement evidence-based solutions. For instance, a hospital might discover that its emergency department has a higher CAUTI rate than its medical wards, prompting a review of catheterization protocols in high-turnover settings. Pairing data with clinical expertise ensures that interventions are both targeted and effective, ultimately improving patient safety and outcomes.
Water Main Break Near Sharp Grossmont Hospital: What You Need to Know
You may want to see also
Explore related products






![]()
Prevalence Data: Percentage of patients with HAIs at a specific point in time
Hospital-acquired infections (HAIs) are a critical public health concern, and understanding their prevalence at specific points in time is essential for targeted interventions. Prevalence data, often expressed as the percentage of patients with HAIs during a given period, provides a snapshot of the burden these infections pose within healthcare settings. For instance, studies have shown that on any given day, approximately 5% to 10% of hospitalized patients in acute care settings may have at least one HAI. This figure varies by region, hospital type, and patient population, with higher rates observed in intensive care units (ICUs), where up to 30% of patients may be affected due to prolonged stays and invasive procedures.
Analyzing prevalence data requires careful consideration of the methodology used to collect it. Point prevalence studies, which assess the number of patients with HAIs at a single point in time, are commonly employed. These studies often categorize HAIs by type, such as surgical site infections, urinary tract infections, or bloodstream infections, providing granular insights into the most common issues. For example, a 2020 European survey found that 20% of HAIs in ICUs were bloodstream infections, highlighting the need for stringent infection control measures in high-risk areas. Such data not only inform resource allocation but also serve as a baseline for evaluating the effectiveness of prevention strategies over time.
From a practical standpoint, healthcare providers can use prevalence data to implement targeted interventions. For instance, if a hospital identifies a 15% prevalence of catheter-associated urinary tract infections (CAUTIs) in a specific ward, it can introduce bundled interventions, such as minimizing catheter use, improving hygiene protocols, and providing staff training. Monitoring prevalence data post-intervention allows for real-time assessment of these measures. Additionally, benchmarking against national or regional averages helps hospitals identify areas for improvement. For example, if a hospital’s HAI prevalence is 12% compared to a national average of 8%, it signals an urgent need for systemic changes.
Comparatively, prevalence data also shed light on disparities in HAI rates across different patient demographics. Studies have shown that older adults, particularly those over 65, are at higher risk, with prevalence rates up to 50% higher than younger patients. Similarly, patients with comorbidities or weakened immune systems are disproportionately affected. Understanding these disparities enables hospitals to tailor interventions, such as enhanced monitoring for high-risk groups or specialized training for staff managing vulnerable populations. For instance, a hospital might introduce daily HAI screening protocols for elderly patients in surgical wards, where prevalence data indicate a higher risk.
In conclusion, prevalence data serve as a vital tool for measuring the immediate impact of HAIs and guiding evidence-based actions. By focusing on the percentage of patients affected at specific points in time, healthcare systems can identify trends, allocate resources effectively, and implement targeted strategies to reduce infection rates. Whether through comparative analysis, demographic-specific interventions, or continuous monitoring, leveraging prevalence data is key to mitigating the burden of HAIs and improving patient outcomes.
Locating Jeferson: A Guide to Morriston Hospital's Department
You may want to see also
Explore related products





![]()
Mortality Statistics: HAI-related death rates and their impact on patient outcomes
Hospital-acquired infections (HAIs) contribute to approximately 99,000 deaths annually in the United States alone, making them a leading cause of mortality in healthcare settings. These infections, ranging from pneumonia to bloodstream infections, are often preventable yet exact a devastating toll on patient outcomes. The mortality rates associated with HAIs vary by infection type, patient demographics, and hospital resources, but one constant remains: their profound impact on survival. For instance, patients with central line-associated bloodstream infections (CLABSIs) face a mortality risk up to 25% higher than those without such infections, underscoring the critical need for targeted interventions.
Analyzing mortality statistics reveals a stark disparity in outcomes based on patient vulnerability. Immunocompromised individuals, the elderly, and those in intensive care units (ICUs) bear the brunt of HAI-related deaths. For example, patients over 65 years old account for nearly 60% of HAI-related fatalities, often due to complications like ventilator-associated pneumonia (VAP). These infections not only increase mortality but also prolong hospital stays, with VAP patients averaging an additional 13 days in the hospital. Such data highlights the dual burden of HAIs: higher death rates and increased healthcare costs.
To mitigate HAI-related mortality, healthcare providers must adopt evidence-based practices. Simple yet effective measures include strict hand hygiene protocols, which can reduce infection rates by up to 50%. Additionally, antimicrobial stewardship programs play a pivotal role in combating antibiotic resistance, a key driver of HAI fatalities. For instance, hospitals that implement such programs have reported a 30% reduction in Clostridioides difficile infections, a common and deadly HAI. These interventions are not just clinical imperatives but ethical obligations to safeguard patient lives.
Comparing global mortality statistics offers further insights into the impact of HAIs. In low-resource settings, where infection control measures are often inadequate, HAI-related death rates can be twice as high as in developed nations. This disparity underscores the importance of investing in healthcare infrastructure and training. For example, the World Health Organization’s Clean Care is Safer Care program has demonstrated significant reductions in HAI rates in participating countries, proving that systemic change can save lives.
Ultimately, mortality statistics serve as a call to action for healthcare systems worldwide. By understanding the data, identifying high-risk populations, and implementing proven strategies, hospitals can drastically reduce HAI-related deaths. The goal is clear: transform these grim statistics into a roadmap for improvement, ensuring that patients leave hospitals healthier, not sicker. Every percentage point reduction in HAI mortality represents countless lives saved and families spared from tragedy.
Vice President Hospitalized: Latest Updates on Their Health Condition
You may want to see also
Explore related products






![]()
Cost Analysis: Financial burden of HAIs on healthcare systems, including treatment and extended stays
Hospital-acquired infections (HAIs) impose a staggering financial burden on healthcare systems, with costs stemming from prolonged hospital stays, additional treatments, and increased resource utilization. Data from the Centers for Disease Control and Prevention (CDC) estimates that HAIs account for approximately $28 billion to $45 billion in excess healthcare costs annually in the United States alone. These infections, ranging from surgical site infections to Clostridioides difficile (C. diff) outbreaks, not only compromise patient safety but also strain hospital budgets, diverting funds from preventive measures and other critical services.
Consider the case of a patient who develops a central line-associated bloodstream infection (CLABSI). Treatment typically involves extended antibiotic therapy, such as a 14-day course of vancomycin (15 mg/kg every 8–12 hours for adults), alongside additional diagnostic tests and intensive monitoring. This scenario can add $30,000 to $50,000 to the patient’s hospital bill, depending on severity. Multiply this by the estimated 30,000 CLABSI cases annually in U.S. hospitals, and the financial impact becomes clear. Extended hospital stays, often averaging 7–10 additional days per HAI case, further exacerbate costs, as each extra day in a hospital bed can range from $2,000 to $4,000.
From a comparative perspective, HAIs disproportionately affect older adults and immunocompromised patients, who often require more intensive interventions. For instance, a 70-year-old patient with a ventilator-associated pneumonia (VAP) may need prolonged mechanical ventilation, broad-spectrum antibiotics like piperacillin-tazobactam (4.5 g every 6 hours), and additional respiratory therapy. This not only increases direct treatment costs but also elevates the risk of complications, such as acute kidney injury, which may necessitate dialysis. Such cases highlight the compounding nature of HAI-related expenses, where one infection can trigger a cascade of costly interventions.
To mitigate this financial burden, healthcare systems must prioritize infection prevention strategies, such as hand hygiene protocols, sterile techniques for invasive procedures, and antimicrobial stewardship programs. For example, implementing a bundled approach to preventing CLABSIs—including daily review of line necessity, chlorhexidine baths, and sterile dressing changes—has been shown to reduce infection rates by up to 70%. While these initiatives require upfront investment, they yield significant long-term savings. A study in *JAMA Internal Medicine* found that hospitals saved an average of $1.3 million annually by reducing HAIs through evidence-based practices.
In conclusion, the financial toll of HAIs extends far beyond individual patient bills, impacting healthcare systems’ ability to allocate resources effectively. By analyzing specific infection types, treatment costs, and prevention strategies, hospitals can develop targeted interventions to reduce both clinical and economic burdens. Practical steps, such as staff training on infection control and leveraging data analytics to identify high-risk areas, are essential. Ultimately, addressing HAIs is not just a clinical imperative but a financial necessity for sustainable healthcare delivery.
Concussion Recovery: Key Signs for Returning to the Hospital
You may want to see also
Explore related products

$81.7 $101.95



$38.34 $62.99


![]()
Trends Over Time: Yearly or quarterly changes in HAI rates and prevention effectiveness
Hospital-acquired infections (HAIs) have shown fluctuating trends over the past decade, with data revealing both progress and persistent challenges. For instance, the Centers for Disease Control and Prevention (CDC) reported a 13% decrease in central line-associated bloodstream infections (CLABSIs) between 2015 and 2019, yet surgical site infections (SSIs) remained relatively stable during the same period. These variations highlight the need for targeted interventions and continuous monitoring. Quarterly data from hospitals in the United Kingdom further illustrates seasonal spikes in HAIs, particularly during winter months, likely due to increased patient volume and staff shortages. Such patterns underscore the importance of resource allocation and preparedness during high-risk periods.
Analyzing prevention effectiveness, hand hygiene compliance rates have emerged as a critical metric. Studies show that hospitals with compliance rates above 80% experience a 30% reduction in HAIs compared to those below 70%. However, maintaining these rates remains a challenge, with compliance often dropping during peak hours or in understaffed units. The implementation of antimicrobial stewardship programs has also shown promise, with a 2021 meta-analysis indicating a 25% decrease in antibiotic-resistant HAIs in hospitals with robust programs. Despite these successes, the rise of multidrug-resistant organisms (MDROs) continues to complicate prevention efforts, necessitating innovative strategies like rapid diagnostic testing and isolation protocols.
A comparative analysis of HAI trends across different healthcare settings reveals disparities in progress. Large academic hospitals tend to outperform smaller community hospitals in reducing HAIs, likely due to greater access to resources and specialized infection control teams. For example, a 2020 study found that CLABSI rates in academic hospitals were 40% lower than in community hospitals. However, smaller facilities have shown significant improvement through collaborative initiatives, such as the CDC’s National Healthcare Safety Network, which provides standardized reporting tools and best practices. This suggests that knowledge-sharing and benchmarking can level the playing field, even for resource-constrained institutions.
Practical steps for hospitals to address these trends include quarterly audits of infection control practices, real-time feedback mechanisms for staff, and patient education on HAI prevention. For instance, a simple yet effective strategy is to post hand hygiene compliance rates in public areas, fostering accountability and friendly competition among units. Additionally, hospitals should prioritize data-driven decision-making by integrating electronic health records (EHRs) with infection surveillance systems. This allows for immediate identification of outbreaks and targeted interventions, such as isolating patients with MDROs or adjusting antibiotic prescribing practices.
In conclusion, the trends in HAI rates and prevention effectiveness over time reveal both achievements and areas for improvement. While certain infection types have seen reductions, others remain stubbornly persistent, and emerging threats like MDROs demand ongoing vigilance. Hospitals must adopt a multifaceted approach, combining evidence-based practices, technological tools, and collaborative efforts to sustain progress. By focusing on quarterly fluctuations, seasonal risks, and setting-specific challenges, healthcare institutions can refine their strategies and ultimately protect more patients from the preventable harm of HAIs.
Psychiatric Hospitals vs. Institutions: What's in a Name?
You may want to see also
Frequently asked questions
Hospital-acquired infections (HAIs) are infections that patients develop while receiving treatment in a hospital, typically after 48 hours of admission. Quantitative data on HAIs includes metrics such as infection rates, incidence per 1,000 patient-days, and the number of cases per specific infection type (e.g., catheter-associated urinary tract infections, surgical site infections).
The incidence rate of HAIs is calculated by dividing the number of new HAI cases by the total number of patient-days (or discharges) and multiplying by a standard factor, often 1,000. For example, if there are 10 HAIs in 10,000 patient-days, the rate is 1 per 1,000 patient-days.
The most common types of HAIs measured quantitatively include central line-associated bloodstream infections (CLABSI), catheter-associated urinary tract infections (CAUTI), surgical site infections (SSI), ventilator-associated pneumonia (VAP), and Clostridioides difficile (C. diff) infections. Each type is tracked using specific rates and metrics.
Hospitals use quantitative data on HAIs to identify trends, compare performance against benchmarks (e.g., CDC’s National Healthcare Safety Network), and implement targeted interventions. Data helps in monitoring the effectiveness of infection prevention strategies, allocating resources, and reducing infection rates over time.