Esophageal manometry is a diagnostic test performed in hospitals to evaluate the function of the esophagus, the muscular tube that connects the mouth to the stomach. This procedure measures the pressure and coordination of esophageal muscle contractions, as well as the relaxation of the lower esophageal sphincter (LES), which controls the passage of food into the stomach. By assessing these factors, esophageal manometry helps diagnose conditions such as achalasia, gastroesophageal reflux disease (GERD), and esophageal motility disorders. The test involves inserting a thin, flexible tube through the nose or mouth into the esophagus, which contains sensors to record pressure changes during swallowing. Results from this test are crucial for determining appropriate treatment plans, including medications, lifestyle changes, or surgical interventions.
| Characteristics | Values |
|---|---|
| Test Name | Esophageal Manometry (also known as Esophageal Motility Study) |
| Purpose | To evaluate the function and pressure of the esophagus and lower esophageal sphincter (LES). |
| Indications | Dysphagia (difficulty swallowing), gastroesophageal reflux disease (GERD), chest pain, suspected motility disorders. |
| Procedure | A thin, flexible tube (catheter) with pressure sensors is passed through the nose into the esophagus. |
| Duration | Typically 30–60 minutes. |
| Preparation | Patients may be asked to fast for 6–8 hours before the test. |
| Anesthesia | Usually not required; local numbing spray may be used for comfort. |
| Risks | Minimal; rare risks include nasal irritation, bleeding, or infection. |
| Results | Measures pressure changes during swallowing to assess esophageal motility and LES function. |
| Diagnosis | Helps diagnose conditions like achalasia, esophageal spasms, or GERD. |
| Follow-Up | Results are interpreted by a gastroenterologist, who may recommend further treatment or tests. |
| Alternative Names | Esophageal Motility Study, Esophageal Pressure Measurement. |
| Latest Advances | High-resolution manometry (HRM) provides more detailed pressure mapping. |
Explore related products






What You'll Learn
- Procedure Overview: Measures esophageal pressure to assess motility and function using a catheter
- Preparation Steps: Fasting, avoiding medications, and informing doctors about allergies or conditions
- During the Test: Catheter insertion through nose, swallowing water, recording pressure changes
- Post-Test Care: Mild discomfort, resume normal activities, report severe pain or issues
- Results Interpretation: Diagnoses conditions like achalasia, GERD, or esophageal spasms
![]()
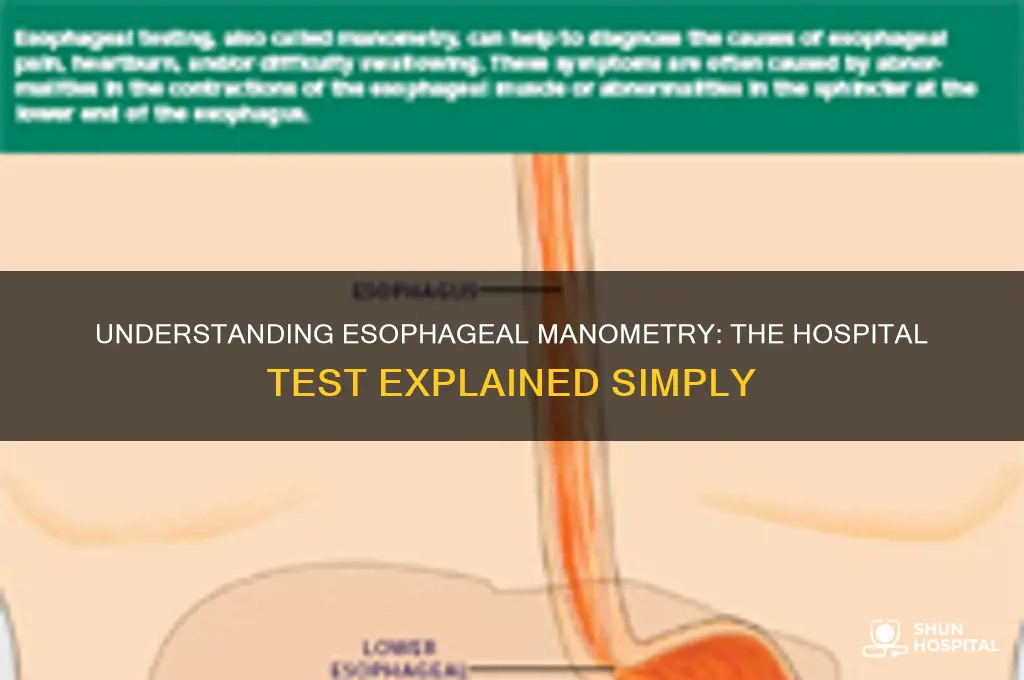
Procedure Overview: Measures esophageal pressure to assess motility and function using a catheter
Esophageal manometry, a diagnostic procedure often shrouded in medical jargon, is essentially a pressure test for your esophagus. Imagine a tiny, flexible tube (catheter) equipped with sensors, gently navigating the path from your nose or mouth, down your throat, and into your esophagus. This catheter acts as a sophisticated pressure gauge, measuring the strength and coordination of the muscular contractions that propel food from your mouth to your stomach.
Think of it as a performance review for your esophagus, assessing its ability to move food efficiently.
The procedure itself is relatively straightforward, though not exactly a walk in the park. You'll be asked to sit upright, and the doctor will guide the catheter into place. While it might trigger a gag reflex initially, local anesthesia can be applied to minimize discomfort. Once in position, you'll be asked to swallow small sips of water, allowing the sensors to record the pressure changes generated by your esophageal muscles. This data is then translated into a visual representation, providing a detailed map of your esophagus's motility.
The entire process typically takes around 30-60 minutes, and while it may be slightly uncomfortable, it's generally well-tolerated.
This test is a crucial tool for diagnosing a range of esophageal disorders. Conditions like achalasia, where the lower esophageal sphincter fails to relax properly, or diffuse esophageal spasm, characterized by uncoordinated muscle contractions, can be identified through the distinct pressure patterns revealed by manometry. By pinpointing the specific motility issue, doctors can tailor treatment plans, which may include medications, dietary modifications, or in some cases, surgical intervention.
It's important to note that esophageal manometry is a specialized test, typically ordered when other diagnostic methods, such as endoscopy or barium swallow, haven't provided conclusive results. If you're experiencing symptoms like difficulty swallowing, chest pain, or frequent heartburn, and standard treatments aren't providing relief, your doctor might recommend this procedure to delve deeper into the underlying cause.
Hospital Calls Your Doctor: Should You Be Concerned?
You may want to see also
Explore related products






![]()
Preparation Steps: Fasting, avoiding medications, and informing doctors about allergies or conditions
Esophageal manometry, a diagnostic test measuring esophageal muscle function, demands meticulous preparation to ensure accuracy and safety. Fasting is paramount; patients must abstain from food and liquids for 6–8 hours prior to the procedure. This clears the esophagus, allowing precise pressure measurements without interference from digestion. Skipping this step risks distorted results, potentially leading to misdiagnosis of conditions like achalasia or gastroesophageal reflux disease (GERD).
Medication management is equally critical. Certain drugs, such as calcium channel blockers, nitrates, or anticholinergics, can alter esophageal motility, skewing test outcomes. Patients should consult their doctor to determine which medications to pause 24–48 hours before the test. For instance, proton pump inhibitors (PPIs) may need temporary discontinuation, though this varies based on the physician’s assessment. Always follow specific instructions, as abrupt medication changes can have health implications.
Allergies and underlying conditions must be disclosed during pre-test consultations. Contrast agents or local anesthetics used during the procedure could trigger reactions in sensitive individuals. Conditions like bleeding disorders, severe GERD, or recent esophageal surgery may require modified protocols or additional precautions. For example, patients with clotting issues might need blood tests beforehand to assess bleeding risks. Transparency ensures tailored care and minimizes complications.
Practical tips enhance compliance: set an alarm to mark the fasting start time, keep water nearby post-fasting for immediate rehydration, and carry a list of medications to the appointment for clarity. For children or elderly patients, caregivers should oversee fasting and medication adjustments to prevent errors. Adhering to these steps not only optimizes the test’s reliability but also safeguards patient well-being during esophageal manometry.
Accessing Cerner from Home: A Guide for Jackson Memorial Hospital Miami Staff
You may want to see also
Explore related products





![]()
During the Test: Catheter insertion through nose, swallowing water, recording pressure changes
Esophageal manometry, a diagnostic procedure to evaluate esophageal motility, involves a series of precise steps that may seem daunting to patients. The process begins with the insertion of a thin, flexible catheter through the nose, a technique that allows for direct access to the esophagus while minimizing discomfort. This catheter, equipped with pressure sensors, is carefully guided down the throat, requiring the patient to remain calm and cooperative. The procedure is typically performed by a trained specialist who ensures the catheter is positioned accurately to capture meaningful data.
Once the catheter is in place, the patient is instructed to swallow small amounts of water at regular intervals. This simple act of swallowing triggers the esophageal muscles to contract, generating pressure changes that are recorded by the sensors. The water acts as a natural stimulus, mimicking the passage of food and providing a realistic assessment of esophageal function. Patients are often advised to swallow slowly and deliberately, allowing the sensors to capture the nuances of muscle activity. This step is critical, as it forms the basis for diagnosing conditions like achalasia or diffuse esophageal spasm.
Recording pressure changes during the test is a highly technical aspect of esophageal manometry. The sensors along the catheter measure the strength and coordination of esophageal contractions, translating these movements into data that can be analyzed later. This real-time monitoring allows healthcare providers to identify abnormalities in motility, such as weak or uncoordinated contractions, which could indicate underlying disorders. The data is typically displayed on a monitor, enabling immediate feedback and adjustments during the procedure. Precision in this phase is key, as even minor discrepancies can significantly impact diagnostic accuracy.
Throughout the test, patient comfort and cooperation are paramount. While the catheter insertion may cause mild discomfort or a gag reflex, the procedure is generally well-tolerated. Patients are encouraged to breathe through their mouths and relax their throat muscles to ease the process. The entire test usually takes 30 to 60 minutes, after which the catheter is gently removed. Post-procedure, patients may experience temporary nasal congestion or a sore throat, but these symptoms typically resolve quickly. Understanding these steps can help alleviate anxiety and ensure a smoother experience during esophageal manometry.
Loma Linda Hospital Murrieta: Private vs. Shared Rooms Explained
You may want to see also
![]()
Post-Test Care: Mild discomfort, resume normal activities, report severe pain or issues
Esophageal manometry, a diagnostic test measuring esophageal muscle function, often leaves patients with mild discomfort post-procedure. This sensation, akin to soreness or a scratchy throat, typically subsides within 24 hours. Patients can expedite relief by gargling warm saltwater or sucking on lozenges, avoiding irritants like spicy foods or alcohol. Understanding this transient discomfort empowers individuals to manage expectations and resume daily routines without undue concern.
Resuming normal activities immediately after esophageal manometry is generally safe, as the test is minimally invasive and does not require sedation. Adults of all age groups can return to work, exercise, and regular diets, though it’s advisable to avoid strenuous activities for the first few hours. Pediatric patients, particularly those under 12, may benefit from a brief rest period to ensure comfort. Practical tips include staying hydrated and opting for soft, easy-to-swallow foods like yogurt or mashed potatoes for the first meal post-test.
While mild discomfort is expected, severe pain, persistent difficulty swallowing, or unusual symptoms like fever or bleeding warrant immediate medical attention. Patients should monitor for signs of infection or complications, such as chest pain or persistent vomiting, and report these to their healthcare provider promptly. A clear understanding of red flags ensures timely intervention, preventing potential complications like esophageal perforation, though such risks are rare, occurring in less than 1% of cases.
Comparatively, post-care for esophageal manometry is simpler than for more invasive procedures like endoscopy, which may require a longer recovery period. Unlike tests involving sedation, patients can drive themselves home and manage their recovery independently. However, adherence to post-test guidelines is crucial, as ignoring severe symptoms can lead to serious health issues. This balance of autonomy and vigilance underscores the importance of patient education in post-procedure care.
Instructive guidance for post-esophageal manometry care includes maintaining a symptom diary for the first 48 hours, noting any unusual sensations or pain levels. Patients should also follow up with their healthcare provider within a week to review test results and address concerns. For those with pre-existing conditions like gastroesophageal reflux disease (GERD), resuming prescribed medications immediately is essential. This structured approach ensures a smooth recovery and facilitates informed discussions about next steps in diagnosis or treatment.
Hospital Rooms: Renting Options and Availability
You may want to see also
![]()
Results Interpretation: Diagnoses conditions like achalasia, GERD, or esophageal spasms
Esophageal manometry, a diagnostic test measuring the pressure and coordination of esophageal muscles, provides critical insights into motility disorders. When interpreting results, clinicians focus on distinct patterns to diagnose conditions like achalasia, GERD, or esophageal spasms. For instance, achalasia is characterized by incomplete lower esophageal sphincter (LES) relaxation and absent peristalsis, often presenting as a "bird’s beak" appearance on barium swallow. Recognizing these patterns is essential for accurate diagnosis and tailored treatment planning.
In contrast to achalasia, GERD (gastroesophageal reflux disease) often shows normal or slightly elevated LES pressure but may reveal impaired peristalsis or increased transient LES relaxations. These findings correlate with the chronic reflux of stomach acid, which damages the esophageal lining. Patients with GERD may also exhibit a "Hill of the Bean" pattern on manometry, indicating delayed esophageal emptying. Understanding these nuances ensures that treatment, such as proton pump inhibitors or lifestyle modifications, is appropriately targeted.
Esophageal spasms, another condition diagnosed via manometry, present as uncoordinated, high-amplitude contractions that fail to propel food effectively. These spasms can be diffuse or localized and are often mistaken for cardiac pain due to their intensity. Manometry results typically show simultaneous or "corkscrew" contractions, distinguishing them from other motility disorders. For patients experiencing these symptoms, calcium channel blockers or nitrates may provide symptomatic relief, but the underlying cause requires careful evaluation.
Interpreting manometry results requires a systematic approach. Clinicians analyze pressure tracings, contraction amplitude, and coordination to differentiate between conditions. For example, a patient with achalasia may require pneumatic dilation or botulinum toxin injection, while GERD management focuses on acid suppression and dietary changes. Esophageal spasms, often idiopathic, may necessitate antispasmodic therapy or psychological interventions for stress-related triggers. Practical tips for patients include maintaining an upright posture after meals and avoiding trigger foods like caffeine or alcohol.
In summary, esophageal manometry serves as a cornerstone in diagnosing motility disorders, with result interpretation hinging on specific pressure and coordination patterns. By identifying conditions like achalasia, GERD, or esophageal spasms, clinicians can devise effective treatment strategies. Patients benefit from tailored interventions, whether pharmacological, procedural, or lifestyle-based, underscoring the test’s role in improving quality of life. Accurate interpretation, coupled with patient education, transforms manometry from a diagnostic tool into a pathway for relief.
Is Panama's Hospital Paitilla Affiliated with Cleveland Clinic?
You may want to see also
Frequently asked questions
Esophageal manometry is a diagnostic test that measures the pressure and coordination of the muscles in the esophagus, the tube that connects the mouth to the stomach.
Esophageal manometry is performed to diagnose conditions related to swallowing difficulties, such as gastroesophageal reflux disease (GERD), achalasia, or esophageal motility disorders.
During the test, a thin, flexible tube with pressure sensors is passed through the nose or mouth into the esophagus. The patient swallows small sips of water while the sensors measure muscle contractions and pressure.
The test is generally not painful but may cause discomfort, such as a gagging sensation or mild soreness in the throat. Local anesthesia or numbing spray may be used to ease the process.
The test typically takes 30 to 60 minutes. Afterward, patients can usually resume normal activities immediately, though they may be advised to avoid eating or drinking for a short period if numbing medication was used. Results are analyzed by a specialist to determine the next steps in treatment.