In hospitals, a critical machine that helps keep a patient's heart beating is the cardiac pacemaker. This small, battery-operated device is often used when a person's heart is unable to maintain a normal rhythm on its own. Implanted under the skin, typically near the collarbone, the pacemaker sends electrical impulses to the heart muscles, ensuring it beats at a steady and appropriate rate. In emergency situations, an external temporary pacemaker may be used, which is a non-invasive or minimally invasive device connected to the patient via electrodes or wires. Both types of pacemakers are life-saving tools, providing essential support for patients with heart rhythm disorders, such as bradycardia, and are closely monitored by healthcare professionals to ensure optimal function.
| Characteristics | Values |
|---|---|
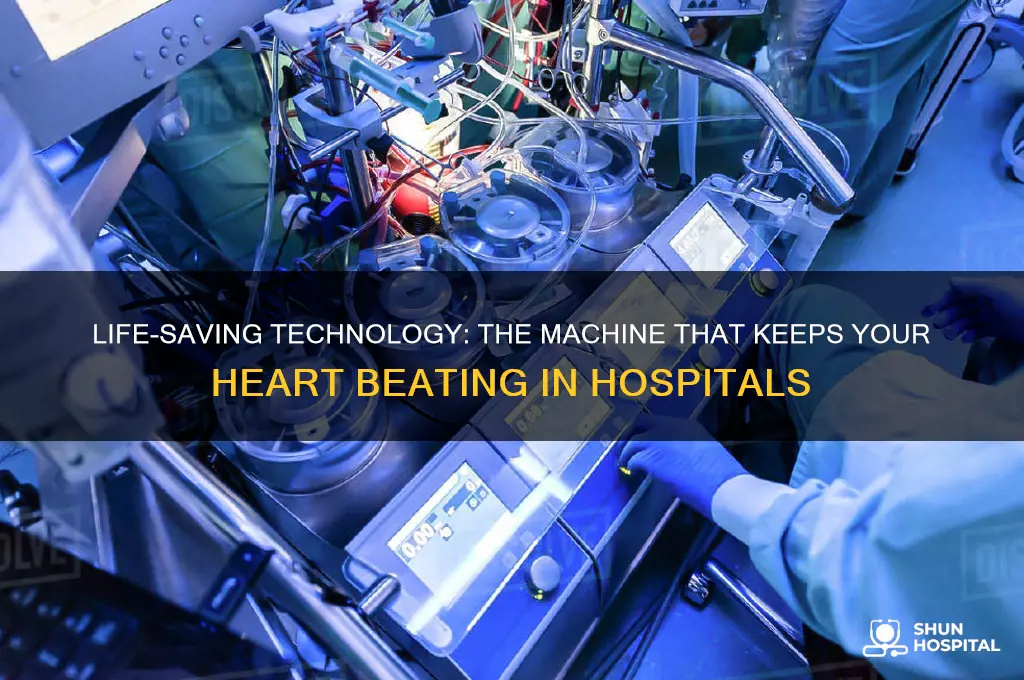
| Name | Cardiac/Heart-Lung Machine or Extracorporeal Membrane Oxygenation (ECMO) |
| Primary Function | Temporarily takes over the function of the heart and lungs. |
| Usage | Open-heart surgery, cardiac arrest, or severe heart/lung failure. |
| Components | Pump, oxygenator, heat exchanger, tubing, and cannulas. |
| Pump Type | Roller or centrifugal pump. |
| Oxygenation | Oxygenator adds oxygen and removes carbon dioxide from blood. |
| Blood Flow Rate | Typically 2-6 liters per minute (adjustable based on patient needs). |
| Temperature Control | Maintains blood temperature between 25°C to 37°C (77°F to 98.6°F). |
| Monitoring | Continuous monitoring of blood pressure, oxygen levels, and flow rate. |
| Duration of Use | Hours to days, depending on the medical condition. |
| Risks | Bleeding, infection, air embolism, and hemolysis. |
| Alternatives | Intra-aortic balloon pump (IABP) or ventricular assist devices (VADs). |
| Latest Advancements | Miniaturized pumps, improved biocompatible materials, and AI monitoring. |
Explore related products






What You'll Learn
- Cardiac Pacemakers: Devices that regulate heart rhythm by sending electrical pulses to the heart muscle
- ECMO Machines: Provide temporary heart and lung support by oxygenating blood outside the body
- Defibrillators: Deliver electric shocks to restore normal heart rhythm during cardiac arrest
- Heart-Lung Bypass: Machines that take over heart and lung function during surgeries like open-heart repair
- Intra-Aortic Balloon Pumps: Assist heart function by increasing blood flow and reducing workload
![]()
Cardiac Pacemakers: Devices that regulate heart rhythm by sending electrical pulses to the heart muscle
In the realm of cardiac care, pacemakers stand as silent sentinels, ensuring the heart's rhythm remains steady and life-sustaining. These small, battery-operated devices are implanted under the skin, typically near the collarbone, and connected to the heart via thin wires called leads. Their primary function is to monitor the heart's electrical activity and deliver precisely timed electrical pulses when necessary, preventing abnormally slow heartbeats (bradycardia) or coordinating the contraction of the heart's chambers in cases of heart block. For instance, a dual-chamber pacemaker can synchronize the right atrium and ventricle, mimicking the heart's natural rhythm more closely than single-chamber models.
Consider the implantation process, which is less invasive than one might assume. Performed under local anesthesia, the procedure typically takes 1–2 hours. The pacemaker's leads are guided through veins into the heart, a process monitored via X-ray. Once positioned, the device is programmed to respond to the patient's specific needs—for example, a minimum heart rate of 60 beats per minute is commonly set. Post-implantation, patients often resume normal activities within a few weeks, though lifting heavy objects or vigorous exercise may be restricted for 4–6 weeks to ensure proper healing.
The longevity of a pacemaker is a critical consideration. Modern devices last 8–15 years, depending on usage and battery type. Lithium-based batteries are standard, with newer models incorporating energy-saving features to extend lifespan. Regular check-ups every 3–6 months are essential to monitor battery status and device function. During these visits, the pacemaker is interrogated using a programmer, a handheld device that communicates wirelessly with the implant. This allows adjustments to pacing settings without surgery—a testament to the device's adaptability.
Despite their life-saving role, pacemakers are not without limitations. Magnetic fields from MRI machines, certain industrial equipment, and even some airport security scanners can interfere with their function. Patients must inform medical and security personnel about their device to avoid complications. Additionally, while pacemakers prevent slow heart rates, they do not shock the heart like defibrillators. For patients at risk of sudden cardiac arrest, a combination device called an implantable cardioverter-defibrillator (ICD) may be recommended instead.
In practice, pacemakers are a cornerstone of treatment for a diverse patient population, from newborns with congenital heart block to elderly individuals with age-related conduction disorders. For example, fetal pacemakers have been used in utero to treat severe bradycardia, showcasing the device's versatility. Advances like leadless pacemakers, inserted via a catheter and positioned directly in the heart, further expand treatment options, particularly for patients at high risk of infection or those with limited vascular access. As technology evolves, pacemakers continue to redefine what it means to keep a heart beating steadily, even in the most challenging circumstances.
Exploring the Eeriest Haunted Old Hospitals Around the World
You may want to see also
Explore related products






![]()
ECMO Machines: Provide temporary heart and lung support by oxygenating blood outside the body
In critical care settings, ECMO (Extracorporeal Membrane Oxygenation) machines serve as a lifeline for patients whose heart and lungs are failing. Unlike traditional ventilators, ECMO directly oxygenates and circulates blood outside the body, bypassing the lungs and heart to allow these organs to rest and heal. This life-sustaining technology is often the last resort for patients with severe respiratory or cardiac failure, such as those with acute respiratory distress syndrome (ARDS) or post-cardiac surgery complications. By mimicking the functions of the heart and lungs, ECMO buys precious time for patients awaiting recovery or transplantation.
The ECMO process begins with the insertion of cannulas into large veins and arteries, typically in the groin or neck. Blood is drawn from the body, pumped through a circuit containing a membrane oxygenator, and then returned to the patient. The oxygenator acts as an artificial lung, removing carbon dioxide and adding oxygen to the blood. Simultaneously, the pump functions as an external heart, maintaining circulation. ECMO can be configured in two modes: veno-venous (VV) for lung support only, or veno-arterial (VA) for both heart and lung support. The choice depends on the patient’s specific needs, with VA ECMO being more invasive but capable of sustaining full cardiopulmonary function.
Despite its life-saving potential, ECMO is not without risks. Patients on ECMO require meticulous monitoring in intensive care units (ICUs), as complications such as bleeding, infection, and clotting are common. Anticoagulants like heparin are administered to prevent blood clots within the circuit, but this increases the risk of bleeding. Additionally, prolonged ECMO use can lead to limb ischemia or stroke. The procedure is resource-intensive, requiring a specialized team of physicians, nurses, and perfusionists. It is typically reserved for patients under 70 years old, as older individuals often face higher complication rates and poorer outcomes.
For families and caregivers, understanding ECMO’s role is crucial. It is not a cure but a bridge—a temporary measure to stabilize patients until their organs recover or a long-term solution, like a transplant, becomes available. The decision to initiate ECMO involves weighing the patient’s overall health, the severity of their condition, and their likelihood of recovery. Clear communication between the medical team and the family is essential, as ECMO often involves prolonged hospital stays and significant emotional and financial burdens.
In practice, ECMO has proven invaluable during crises like the COVID-19 pandemic, where it was used to support patients with severe pneumonia and ARDS. However, its success depends on timely intervention and expert management. Hospitals must invest in ECMO infrastructure and training to maximize its benefits. For patients, ECMO represents a fragile but vital connection to life, offering hope when all other options have been exhausted. Its complexity underscores the marvels of modern medicine, even as it reminds us of the delicate balance between innovation and human vulnerability.
Easy Steps to Connect to Wi-Fi at Jacksonville Memorial Hospital
You may want to see also
Explore related products






![]()
Defibrillators: Deliver electric shocks to restore normal heart rhythm during cardiac arrest
In the critical moments of cardiac arrest, every second counts, and defibrillators are the unsung heroes that can mean the difference between life and death. These devices deliver a measured electric shock to the heart, interrupting chaotic electrical activity and allowing the heart’s natural pacemaker to reestablish a normal rhythm. Unlike pacemakers, which provide ongoing support for irregular heartbeats, defibrillators are designed for emergency intervention during sudden cardiac arrest, where the heart’s electrical system fails catastrophically. They are a cornerstone of resuscitation efforts, used in hospitals, ambulances, and public spaces, ensuring that immediate action can be taken when time is of the essence.
The process of using a defibrillator is both precise and urgent. First, electrodes are attached to the patient’s chest, either via adhesive pads or handheld paddles, to assess the heart’s rhythm. If a shockable rhythm—ventricular fibrillation or pulseless ventricular tachycardia—is detected, the device charges to a specific energy level, typically between 120 and 360 joules for adults, depending on the protocol. For children, the dosage is weight-based, often starting at 2 to 4 joules per kilogram. Once charged, a shock is delivered, either manually by a trained operator or automatically in the case of an automated external defibrillator (AED). This jolt temporarily stops the heart’s electrical activity, giving it a chance to reset and resume a normal beat.
While defibrillators are life-saving, their use requires careful consideration. Not all cardiac arrests are shockable; asystole (flatline) and pulseless electrical activity (PEA) do not respond to defibrillation. Misuse can cause unnecessary harm, such as burns or tissue damage, though modern devices are designed with safety features to minimize risks. Training is crucial—whether for healthcare professionals or bystanders using public AEDs—as proper placement of pads, timing of shocks, and coordination with CPR are critical for success. Regular maintenance of the device, including battery checks and pad expiration monitoring, ensures it functions when needed.
The evolution of defibrillators has made them more accessible and user-friendly. AEDs, for instance, provide voice prompts and visual instructions, enabling even untrained individuals to administer shocks effectively. In hospitals, advanced models like implantable cardioverter-defibrillators (ICDs) offer long-term protection for high-risk patients, automatically detecting and correcting life-threatening arrhythmias. These innovations highlight how technology has transformed defibrillators from specialized tools into widely available instruments of survival, bridging the gap between medical expertise and immediate public intervention.
Ultimately, defibrillators are a testament to the power of medical technology in saving lives. Their ability to restore normal heart rhythm in moments of crisis underscores their indispensability in emergency care. Whether in a hospital setting or a public space, understanding their function, limitations, and proper use empowers individuals to act decisively during cardiac arrest. In the race against time, defibrillators are not just machines—they are lifelines.
Carolina Hospital Florence SC: Location Guide for Easy Access
You may want to see also
Explore related products






![]()
Heart-Lung Bypass: Machines that take over heart and lung function during surgeries like open-heart repair
During complex cardiac surgeries, the heart-lung bypass machine, also known as the cardiopulmonary bypass (CPB) machine, becomes the patient's temporary heart and lungs. This sophisticated device takes over the vital functions of oxygenating blood and circulating it throughout the body, allowing surgeons to operate on a still, bloodless heart. The CPB machine consists of several key components: a pump to circulate blood, an oxygenator to add oxygen and remove carbon dioxide, and a series of tubes and filters to ensure the blood remains clean and at the correct temperature. Without this technology, many life-saving cardiac procedures, such as coronary artery bypass grafting or valve repairs, would be impossible.
Operating the heart-lung bypass machine requires precision and constant monitoring. Before initiating bypass, the perfusionist—a specialized healthcare professional—connects the patient to the machine by inserting cannulas into the heart and major blood vessels. The blood is then diverted through the CPB circuit, where it is oxygenated and returned to the body. Throughout the procedure, the perfusionist adjusts flow rates, typically maintaining a cardiac output of 2.2 to 2.5 liters per minute per square meter of body surface area, and monitors parameters like oxygen saturation, hematocrit, and electrolyte levels. This real-time management ensures the patient remains stable while the surgeon works on the heart.
One of the critical challenges of heart-lung bypass is minimizing its impact on the body. Prolonged use of the CPB machine can lead to complications such as inflammation, blood clotting, or organ damage. To mitigate these risks, modern machines incorporate features like biocompatible coatings on circuits and filters to reduce blood trauma. Additionally, surgeons often limit bypass time to under 120 minutes, as longer durations correlate with increased morbidity. Patients, especially those over 70 or with pre-existing conditions, may require tailored strategies, such as mild hypothermia (lowering body temperature to 32–34°C) to protect tissues during bypass.
Despite its complexity, the heart-lung bypass machine has revolutionized cardiac surgery, enabling procedures that were once considered too risky. For instance, during an open-heart repair, the machine allows surgeons to arrest the heart completely, providing a motionless field for precise suturing or grafting. Post-bypass, the patient is gradually weaned off the machine as their heart and lungs resume function. Recovery from CPB varies; some patients may experience temporary confusion or fatigue due to the inflammatory response, but most regain full cognitive and physical function within days. This technology underscores the synergy between engineering and medicine, transforming what was once a fatal condition into a treatable one.
Understanding Select Specialty Hospital: A Comprehensive Long-Term Care Facility
You may want to see also
Explore related products






![]()
Intra-Aortic Balloon Pumps: Assist heart function by increasing blood flow and reducing workload
In critical care settings, the intra-aortic balloon pump (IABP) stands as a vital tool for patients with compromised heart function. This device operates on a simple yet ingenious principle: a balloon inserted into the aorta inflates and deflates in sync with the heart’s rhythm. During diastole (when the heart relaxes), the balloon inflates, increasing blood flow to the coronary arteries and reducing the heart’s workload. During systole (when the heart contracts), it deflates, decreasing afterload and easing the heart’s pumping effort. This dual action makes the IABP particularly effective for patients recovering from acute myocardial infarction, undergoing high-risk cardiac surgery, or experiencing cardiogenic shock.
Consider the mechanics: the IABP is connected to a console that monitors and adjusts the balloon’s timing based on the patient’s ECG. The balloon is typically inserted via the femoral artery and positioned in the descending aorta. Optimal placement is critical—too high, and it may obstruct coronary arteries; too low, and it loses effectiveness. The inflation-deflation ratio is usually set at 1:1, meaning the balloon cycles once per heartbeat. For patients with specific needs, such as those with arrhythmias, the ratio may be adjusted to 1:2 or 1:3. Nurses and physicians must closely monitor for complications like limb ischemia, infection, or balloon rupture, though these are rare with proper management.
From a clinical perspective, the IABP’s benefits are clear but not without limitations. It can increase cardiac output by up to 30% and reduce myocardial oxygen demand by 20–30%, making it a lifeline for patients with severely reduced ejection fractions (below 30%). However, it is not a long-term solution; most patients remain on the device for 24–72 hours, though some may require it for up to a week. Contraindications include severe aortic valve disease, active bleeding, or peripheral vascular disease, as these conditions increase the risk of complications. For eligible patients, the IABP serves as a bridge to recovery or more definitive interventions like coronary artery bypass grafting or heart transplantation.
Practical tips for healthcare providers include ensuring adequate anticoagulation to prevent thrombosis, typically with a heparin infusion targeting an activated partial thromboplastin time (aPTT) of 50–70 seconds. Regular assessments of distal pulses and skin perfusion in the lower extremities are essential to detect early signs of ischemia. Patients should be positioned to avoid kinking the IABP catheter, and the device’s alarm system must be continuously monitored for malfunctions. While the IABP is not a cure, its ability to stabilize hemodynamics and buy time for the heart to recover makes it an indispensable tool in the cardiac care arsenal.
In summary, the intra-aortic balloon pump is a sophisticated yet practical intervention for patients with acute heart failure. Its mechanism of action—increasing diastolic blood flow and reducing systolic afterload—addresses the core challenges of a struggling heart. While it requires careful management and is not suitable for all patients, its role in critical care is undeniable. For clinicians, understanding its operation, indications, and limitations ensures its effective use, potentially saving lives in the most precarious moments.
How to Say 'They Brought Me to the Hospital' in Different Languages
You may want to see also
Frequently asked questions
The machine that keeps your heart beating in the hospital is called a cardiac pacemaker. It is a small device that sends electrical impulses to the heart to maintain a regular heartbeat when the heart’s natural rhythm is disrupted.
Yes, a ventricular assist device (VAD) or an extracorporeal membrane oxygenation (ECMO) machine can take over or support the heart’s function in critical situations, such as heart failure or during surgery.
A defibrillator delivers a high-energy electric shock to the heart to restore its normal rhythm in cases of life-threatening arrhythmias, such as ventricular fibrillation or cardiac arrest.
While machines like ECMO or VADs can temporarily support or partially replace the heart’s function, they cannot permanently replace the heart. In some cases, a heart-lung machine may be used during open-heart surgery to take over the heart and lung functions temporarily.































