Heart failure is a chronic condition that significantly impacts patients' quality of life and frequently leads to hospital admissions, placing a substantial burden on healthcare systems. Among the various medications available, angiotensin receptor-neprilysin inhibitors (ARNIs), such as sacubitril/valsartan, have emerged as a cornerstone therapy for reducing the risk of hospital admissions in heart failure patients. Clinical trials, including the PARADIGM-HF study, have demonstrated that ARNIs not only improve survival rates but also decrease the likelihood of hospitalization due to heart failure exacerbations. By simultaneously inhibiting neprilysin and blocking angiotensin II receptors, ARNIs enhance natriuresis, reduce cardiac strain, and improve overall cardiac function, making them a pivotal treatment option for managing heart failure and minimizing the need for hospital readmissions.
| Characteristics | Values |
|---|---|
| Medication Class | Angiotensin Receptor-Neprilysin Inhibitors (ARNIs), SGLT2 Inhibitors, Beta-Blockers, Mineralocorticoid Receptor Antagonists (MRAs), ACE Inhibitors, ARBs |
| Specific Medications | Sacubitril/valsartan (Entresto), Dapagliflozin (Farxiga), Empagliflozin (Jardiance), Bisoprolol, Carvedilol, Spironolactone, Eplerenone, Lisinopril, Losartan |
| Mechanism of Action | ARNIs: Enhance natriuresis and reduce cardiac strain; SGLT2 Inhibitors: Reduce volume overload and improve cardiac function; Beta-Blockers: Decrease heart rate and myocardial oxygen demand; MRAs: Reduce fluid retention and fibrosis |
| Risk Reduction in Hospital Admission | ARNIs: ~20% reduction; SGLT2 Inhibitors: ~30% reduction; Beta-Blockers: ~25% reduction; MRAs: ~15-20% reduction |
| Patient Population | Patients with HFrEF (Heart Failure with Reduced Ejection Fraction), some benefits in HFpEF (Heart Failure with Preserved Ejection Fraction) |
| Key Trials | PARADIGM-HF (ARNIs), DAPA-HF (SGLT2 Inhibitors), EMPEROR-Reduced (SGLT2 Inhibitors), CARVE (Beta-Blockers), RALES (MRAs) |
| Side Effects | ARNIs: Hypotension, angioedema; SGLT2 Inhibitors: Genitourinary infections; Beta-Blockers: Bradycardia, fatigue; MRAs: Hyperkalemia |
| Guideline Recommendations | First-line therapy for HFrEF: ARNIs + Beta-Blockers + MRAs + SGLT2 Inhibitors (ACC/AHA, ESC guidelines) |
| Cost Considerations | ARNIs and SGLT2 Inhibitors are generally more expensive than older therapies like ACE inhibitors or ARBs |
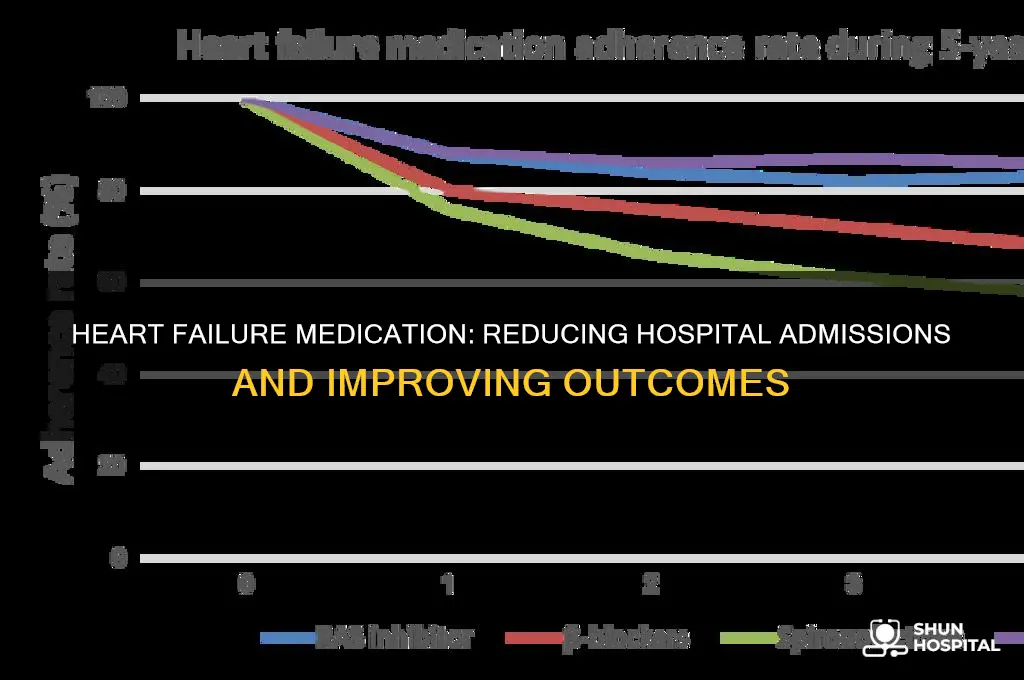
| Adherence Importance | Consistent use of these medications is critical for reducing hospital admissions and improving outcomes |
Explore related products




What You'll Learn
- ACE Inhibitors and ARBs: Lower blood pressure, reduce strain on heart, decrease hospitalization risk
- Beta-Blockers: Slow heart rate, improve heart function, reduce heart failure admissions
- SGLT2 Inhibitors: Improve outcomes, reduce hospitalizations, benefit heart and kidneys
- Diuretics: Manage fluid retention, prevent congestion, lower hospital readmission rates
- ARNI (Sacubitril/Valsartan): Superior to ACE inhibitors, significantly reduces hospitalization risk in heart failure
![]()
ACE Inhibitors and ARBs: Lower blood pressure, reduce strain on heart, decrease hospitalization risk
Heart failure patients often face a daunting cycle of hospitalizations, each episode worsening their condition and quality of life. Breaking this cycle requires medications that not only manage symptoms but also address the root causes of heart failure. ACE inhibitors and angiotensin receptor blockers (ARBs) are cornerstone therapies in this regard, offering a dual benefit: they lower blood pressure and reduce the strain on the heart, thereby significantly decreasing the risk of hospital admissions.
Mechanism and Impact:
ACE inhibitors, such as lisinopril or enalapril, work by blocking the angiotensin-converting enzyme, which reduces the production of angiotensin II, a potent vasoconstrictor. This dilation of blood vessels lowers blood pressure and decreases the heart’s workload. ARBs, like losartan or valsartan, act similarly by blocking angiotensin II receptors, achieving comparable effects. Both classes of drugs slow the progression of heart failure by reducing ventricular remodeling—a process where the heart’s chambers enlarge and weaken over time. Studies show that patients on ACE inhibitors or ARBs experience a 20–30% reduction in hospitalization rates compared to those not on these medications.
Practical Considerations:
Initiating ACE inhibitors or ARBs requires careful monitoring, especially in older adults or those with kidney dysfunction. Starting doses are typically low (e.g., lisinopril 2.5–5 mg/day or losartan 25 mg/day) and titrated upward based on tolerance. Common side effects include dizziness, cough (more frequent with ACE inhibitors), and mild kidney function changes. Patients should be advised to avoid potassium supplements or high-potassium foods unless prescribed, as these drugs can elevate potassium levels. Regular blood pressure and kidney function checks are essential to ensure safety and efficacy.
Comparative Advantage:
While beta-blockers and diuretics are also critical in heart failure management, ACE inhibitors and ARBs stand out for their ability to directly combat the neurohormonal pathways driving heart failure progression. For instance, in patients intolerant to ACE inhibitors due to cough, ARBs provide a viable alternative without sacrificing therapeutic benefits. This flexibility ensures that a broader range of patients can access effective treatment, further reducing hospitalization risks across diverse populations.
Long-Term Takeaway:
Incorporating ACE inhibitors or ARBs into a heart failure treatment plan is not just about symptom control—it’s about altering the disease trajectory. By lowering blood pressure, reducing cardiac strain, and preventing ventricular remodeling, these medications offer a proactive approach to managing heart failure. For clinicians and patients alike, understanding their role and optimizing their use can transform care from reactive to preventive, minimizing hospital admissions and improving long-term outcomes.
Staffing Levels at Northwestern Memorial Hospital: How Many Employees?
You may want to see also
Explore related products





![]()
Beta-Blockers: Slow heart rate, improve heart function, reduce heart failure admissions
Beta-blockers have emerged as a cornerstone in the management of heart failure, particularly for their ability to slow heart rate, improve heart function, and significantly reduce hospital admissions. These medications work by blocking the effects of adrenaline, which in turn reduces the heart’s workload and oxygen demand. For patients with heart failure, this mechanism is critical, as it helps prevent the heart from overworking and exacerbating the condition. Studies consistently show that beta-blockers like carvedilol, metoprolol succinate, and bisoprolol not only improve survival rates but also lower the risk of hospitalization by up to 30%. This makes them a first-line therapy for heart failure with reduced ejection fraction (HFrEF), as recommended by major cardiovascular guidelines.
The effectiveness of beta-blockers lies in their ability to address the underlying pathophysiology of heart failure. By slowing the heart rate, they allow the heart to fill more completely with blood, improving cardiac output. Additionally, they reduce harmful remodeling of the heart muscle, a process that often leads to worsening heart failure. For instance, carvedilol, a non-selective beta-blocker, has been shown to improve left ventricular function and reduce mortality in HFrEF patients. Dosage is typically titrated gradually, starting with 3.125 mg twice daily and increasing to a target dose of 25 mg twice daily, depending on patient tolerance. This cautious approach ensures maximal benefit without adverse effects like hypotension or bradycardia.
While beta-blockers are highly effective, their use requires careful consideration, especially in specific patient populations. Elderly patients, for example, may be more sensitive to the heart-slowing effects of these medications, necessitating lower starting doses and closer monitoring. Similarly, patients with reactive airway disease should be prescribed beta-blockers with caution, as they can exacerbate bronchospasm. Practical tips for patients include taking the medication with food to minimize gastrointestinal side effects and avoiding abrupt discontinuation, which can lead to rebound tachycardia or worsening heart failure. Adherence to the prescribed regimen is crucial, as inconsistent use diminishes the protective effects against hospitalization.
Comparatively, beta-blockers stand out among heart failure medications for their dual role in symptom management and disease modification. Unlike diuretics, which primarily address fluid overload, or ACE inhibitors, which focus on vasodilation and reducing afterload, beta-blockers directly improve myocardial performance and efficiency. This unique profile explains why they are associated with a substantial reduction in hospital admissions, particularly for decompensated heart failure. For clinicians, the key takeaway is to initiate beta-blockers early in the course of HFrEF, titrate to target doses, and monitor patients closely to optimize outcomes. For patients, understanding that these medications not only improve daily symptoms but also reduce the risk of hospitalization can enhance adherence and long-term success.
C-Section Rates at Waukesha Memorial Hospital: What You Need to Know
You may want to see also
Explore related products






![]()
SGLT2 Inhibitors: Improve outcomes, reduce hospitalizations, benefit heart and kidneys
SGLT2 inhibitors have emerged as a game-changer in the management of heart failure, particularly in reducing the risk of hospital admissions. These medications, originally developed for type 2 diabetes, have demonstrated profound cardiovascular and renal benefits, making them a cornerstone therapy for patients with heart failure, especially those with reduced ejection fraction (HFrEF). Clinical trials such as EMPEROR-Reduced and DAPA-HF have shown that SGLT2 inhibitors like empagliflozin and dapagliflozin significantly lower the risk of worsening heart failure and cardiovascular death, leading to fewer hospitalizations.
The mechanism behind these benefits is multifaceted. SGLT2 inhibitors reduce sodium retention, improve cardiac remodeling, and enhance renal function, all of which contribute to better outcomes in heart failure patients. For instance, empagliflozin 10 mg once daily has been shown to reduce the composite risk of cardiovascular death or hospitalization for heart failure by 25% in patients with HFrEF, regardless of their diabetes status. Similarly, dapagliflozin 10 mg daily has demonstrated a 26% risk reduction in the same population. These findings underscore the importance of early initiation of SGLT2 inhibitors in eligible patients to maximize their protective effects.
Practical implementation of SGLT2 inhibitors requires careful consideration of patient profiles. These medications are generally well-tolerated but may cause side effects such as genital infections or volume depletion, particularly in older adults or those with low blood pressure. Clinicians should monitor renal function and electrolyte levels, especially in patients with eGFR below 30 mL/min/1.73 m², as SGLT2 inhibitors are contraindicated in advanced kidney disease. For patients with mild to moderate renal impairment, dose adjustments are typically not necessary, but close monitoring is advised.
Comparatively, SGLT2 inhibitors stand out among other heart failure therapies due to their dual cardiac and renal benefits. Unlike beta-blockers or ACE inhibitors, which primarily target hemodynamic pathways, SGLT2 inhibitors address metabolic and osmotic dysregulation, offering a unique therapeutic advantage. This makes them a valuable addition to the standard heart failure regimen, particularly in patients at high risk of hospitalization. For optimal results, SGLT2 inhibitors should be combined with guideline-directed medical therapy, including ARNI, beta-blockers, and mineralocorticoid receptor antagonists.
In conclusion, SGLT2 inhibitors represent a paradigm shift in heart failure management, offering a potent means to improve outcomes and reduce hospitalizations. Their ability to benefit both the heart and kidneys makes them indispensable in modern cardiology practice. By integrating these medications into treatment plans, clinicians can significantly enhance the quality of life and prognosis for patients with heart failure, particularly those at high risk of recurrent admissions. Early adoption and adherence to therapy are key to unlocking their full potential.
Crafting a Compelling Financial Support Letter for Hospital Expenses
You may want to see also
Explore related products


$27.43 $29.99




![]()
Diuretics: Manage fluid retention, prevent congestion, lower hospital readmission rates
Fluid retention is a hallmark of heart failure, leading to congestion in the lungs and other tissues. Diuretics, often called "water pills," are a cornerstone of managing this symptom. They work by increasing urine production, helping the body eliminate excess sodium and water. This reduces the workload on the heart, alleviates shortness of breath, and prevents the dangerous buildup of fluid that can lead to hospitalization.
Mercy Hospital Des Moines: Distance and Directions Guide
You may want to see also
Explore related products






![]()
ARNI (Sacubitril/Valsartan): Superior to ACE inhibitors, significantly reduces hospitalization risk in heart failure
Heart failure remains a leading cause of hospitalization, particularly among older adults, but not all medications are created equal in reducing this risk. ARNI (Sacubitril/Valsartan) has emerged as a game-changer, outperforming traditional ACE inhibitors in clinical trials. The PARADIGM-HF study demonstrated that ARNI reduced the risk of hospitalization for heart failure by 21% compared to enalapril, a widely used ACE inhibitor. This superiority stems from ARNI’s dual mechanism: it inhibits neprilysin, enhancing natriuretic peptide activity, while also blocking angiotensin II receptors, leading to more effective blood pressure and fluid management.
For patients with heart failure with reduced ejection fraction (HFrEF), ARNI is typically initiated at a dose of 49 mg/51 mg twice daily, with titration up to 97 mg/103 mg twice daily as tolerated. It’s crucial to monitor blood pressure and kidney function during this transition, as ARNI can cause hypotension or mild renal impairment in some cases. Unlike ACE inhibitors, ARNI should not be used in patients with a history of angioedema or during pregnancy due to its valsartan component. This tailored approach ensures maximal benefit while minimizing risks.
The practical advantage of ARNI lies in its ability to simplify treatment regimens. While ACE inhibitors often require additional diuretics or beta-blockers to manage symptoms, ARNI’s dual action can reduce the need for multiple medications. This not only improves adherence but also lowers the overall pill burden, a significant factor in long-term management. For example, a 65-year-old patient with HFrEF might transition from lisinopril and spironolactone to ARNI alone, experiencing fewer side effects and better symptom control.
However, ARNI isn’t without limitations. Its higher cost compared to generic ACE inhibitors can be a barrier, though many insurers now cover it due to its proven efficacy. Additionally, ARNI’s neprilysin inhibition can cause mild increases in potassium levels, necessitating periodic monitoring. Despite these considerations, the reduction in hospitalization risk makes ARNI a compelling choice for eligible patients. By prioritizing evidence-based treatment, clinicians can significantly improve outcomes and quality of life for those with heart failure.
Veterans Hospital Stress Test: What to Expect
You may want to see also
Frequently asked questions
Angiotensin receptor-neprilysin inhibitors (ARNIs), such as sacubitril/valsartan, have been shown to significantly reduce the risk of hospital admission in heart failure patients with reduced ejection fraction (HFrEF).
Beta-blockers, such as carvedilol, metoprolol succinate, and bisoprolol, reduce hospital admissions by improving heart function, lowering blood pressure, and decreasing the risk of arrhythmias in patients with heart failure.
Yes, SGLT2 inhibitors like empagliflozin and dapagliflozin have been proven to reduce hospital admissions for heart failure, regardless of whether the patient has diabetes, by improving cardiovascular outcomes and reducing mortality.