Hospital-acquired urinary tract infections (UTIs) are a significant concern in healthcare settings, with a substantial proportion directly linked to the use of urinary catheters. Studies indicate that catheter-associated UTIs account for approximately 70-80% of all hospital-acquired UTIs, making them the most common type of healthcare-associated infection. This high prevalence is primarily due to the prolonged use of catheters, which disrupts the natural urinary tract defenses and provides a pathway for bacteria to enter the bladder. Understanding this statistic is crucial for implementing targeted infection prevention strategies, such as minimizing unnecessary catheter use, improving insertion techniques, and ensuring proper maintenance to reduce patient morbidity and healthcare costs.
| Characteristics | Values |
|---|---|
| Percentage of Hospital-Acquired UTIs from Catheters | Approximately 75-80% of hospital-acquired UTIs are catheter-associated (CAUTIs). |
| Primary Risk Factor | Urinary catheterization is the most significant risk factor for hospital-acquired UTIs. |
| Duration of Catheterization | Risk of CAUTI increases by 3-10% per day of catheter use. |
| Prevention Strategies | Proper insertion techniques, aseptic practices, and timely removal. |
| Annual CAUTI Cases (U.S.) | Estimated 100,000-400,000 cases annually in U.S. hospitals. |
| Economic Impact | CAUTIs contribute to $400 million-$1 billion in healthcare costs annually. |
| Mortality Rate Associated with CAUTIs | Up to 13% of patients with CAUTIs may develop sepsis, leading to increased mortality. |
| Common Pathogens | E. coli, Klebsiella, Pseudomonas, and Enterococcus are frequently isolated. |
| Prevention Guidelines | CDC and WHO emphasize minimizing catheter use and maintaining hygiene. |
Explore related products





What You'll Learn
![]()
Catheter-associated UTI prevalence in hospitals
Urinary tract infections (UTIs) are among the most common hospital-acquired infections, with catheterization playing a significant role in their development. Studies indicate that catheter-associated UTIs (CAUTIs) account for approximately 75% to 80% of all hospital-acquired UTIs, making them a critical focus for infection prevention strategies. This prevalence is largely due to the direct pathway catheters provide for bacteria to enter the urinary tract, bypassing the body’s natural defenses. Understanding this statistic underscores the urgent need for healthcare providers to optimize catheter use and care protocols.
From an analytical perspective, the high prevalence of CAUTIs highlights systemic issues in catheter management. Prolonged and unnecessary catheterization is a primary risk factor, as each additional day of use increases infection risk by 3% to 7%. Hospitals often struggle with balancing the clinical necessity of catheters against the risks they pose. For instance, in intensive care units (ICUs), where catheterization rates can exceed 80%, CAUTI rates are disproportionately higher compared to general wards. Addressing this disparity requires evidence-based practices, such as implementing catheter insertion bundles and daily assessments for removal.
Instructively, reducing CAUTI prevalence begins with strict adherence to aseptic techniques during catheter insertion. Healthcare providers should use sterile gloves, drapes, and lubricants, and ensure proper hand hygiene before and after the procedure. Once inserted, catheters must be secured to prevent movement and maintained with a closed drainage system. Patients and families can also play a role by advocating for timely removal and questioning the necessity of prolonged catheterization. For example, a simple checklist for catheter care can reduce CAUTI rates by up to 50% in some settings.
Comparatively, CAUTI rates vary significantly across hospitals and regions, reflecting differences in practice and resource availability. In the United States, CAUTI rates in acute care hospitals range from 1.0 to 4.0 per 1,000 catheter days, while in low-resource settings, these rates can be substantially higher due to limited access to sterile supplies and training. This disparity emphasizes the need for globally scalable interventions, such as low-cost catheter care kits and standardized training programs. By learning from high-performing hospitals, others can adopt proven strategies to reduce CAUTI prevalence.
Descriptively, the impact of CAUTIs extends beyond clinical outcomes, imposing substantial financial and emotional burdens. Treating a single CAUTI can cost hospitals $800 to $2,000, with prolonged hospital stays and potential complications like sepsis further inflating expenses. For patients, CAUTIs can lead to discomfort, anxiety, and decreased quality of life. Imagine a 72-year-old patient admitted for a routine surgery, only to develop a CAUTI that extends their hospital stay by a week. Such scenarios are preventable with proactive measures, such as using antimicrobial catheters or limiting catheter use to high-risk patients.
In conclusion, the prevalence of catheter-associated UTIs in hospitals is a preventable yet pervasive issue. By focusing on evidence-based practices, education, and resource allocation, healthcare systems can significantly reduce CAUTI rates. Hospitals must prioritize catheter stewardship, ensuring that every insertion is justified and every day of use is necessary. With concerted effort, the percentage of hospital-acquired UTIs attributed to catheters can be drastically reduced, improving patient safety and outcomes.
Is Great Ormond Street Hospital Affected by London's Congestion Charge?
You may want to see also
Explore related products



![Foley Catheter Stabilization Device [2-Pack] – Gentle Securement with Teksil Lock, 360° Swivel Tab, Waterproof Silicone Adhesive, No Skin Prep Needed & Painless Removal](https://m.media-amazon.com/images/I/51Txi8ArwGL._AC_UL320_.jpg)


![]()
Risk factors for catheter-induced infections
Catheter-associated urinary tract infections (CAUTIs) account for approximately 75-80% of all hospital-acquired UTIs, making them a critical focus in infection prevention. Understanding the risk factors is essential for minimizing patient harm and healthcare costs. One primary risk factor is the duration of catheterization. The longer a urinary catheter remains in place, the higher the likelihood of bacterial colonization and subsequent infection. For instance, the risk of CAUTI increases by 3-10% per day of catheter use. Clinicians should adhere to guidelines recommending catheter removal as soon as medically appropriate, typically within 24-48 hours if not clinically indicated.
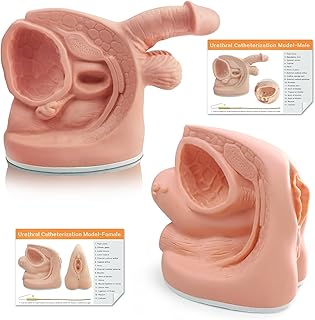
Another significant risk factor is improper catheter insertion and maintenance. Contamination during insertion can introduce pathogens directly into the urinary tract. Healthcare providers must follow strict aseptic techniques, including hand hygiene, sterile gloves, and cleaning the urethral meatus with antiseptic solutions. Additionally, ensuring the catheter is securely positioned and the drainage system remains unobstructed is crucial. For example, kinking or disconnection of the tubing can lead to urine backflow, increasing infection risk. Regular monitoring and patient education on catheter care can mitigate these risks.
Patient-specific factors also play a pivotal role in CAUTI susceptibility. Elderly patients, particularly those over 65, are at higher risk due to age-related immune system decline and increased likelihood of underlying conditions like diabetes or renal impairment. Similarly, individuals with compromised immune systems, such as those undergoing chemotherapy or living with HIV, face elevated risks. Healthcare providers should assess these vulnerabilities and tailor preventive strategies accordingly, such as using antimicrobial-coated catheters for high-risk patients.
Lastly, the type of catheter used can influence infection rates. Latex catheters, for instance, may cause allergic reactions and tissue irritation, increasing susceptibility to infection. Silicone or hydrogel-coated catheters are often preferred for their biocompatibility and reduced friction during insertion. For long-term catheterization, closed systems with pre-connected drainage bags are recommended to minimize manipulation and exposure to pathogens. Selecting the appropriate catheter type based on patient needs and clinical context is a critical step in reducing CAUTI incidence.
In summary, reducing catheter-induced infections requires a multifaceted approach targeting duration of use, insertion practices, patient-specific risks, and catheter selection. By addressing these factors systematically, healthcare providers can significantly lower CAUTI rates, improving patient outcomes and reducing the burden on healthcare systems. Practical steps, such as adhering to evidence-based guidelines and leveraging advanced catheter technologies, are key to achieving this goal.
Ekmwood Park to Hackensack Hospital: Quick Mileage Guide
You may want to see also
Explore related products






![]()
Prevention strategies for catheter UTIs
Catheter-associated urinary tract infections (CAUTIs) account for approximately 75-80% of all hospital-acquired UTIs, making them a critical focus for prevention strategies. This staggering statistic underscores the urgent need for targeted interventions to reduce patient harm and healthcare costs. By implementing evidence-based practices, healthcare providers can significantly lower the incidence of these preventable infections.
Step 1: Minimize Unnecessary Catheter Use
The most effective prevention strategy is to avoid catheterization when possible. Catheters should only be inserted for clear, evidence-based indications, such as acute urinary retention, perioperative use in specific surgeries, or critical care monitoring. Alternatives like intermittent catheterization or bedside ultrasound to assess bladder volume can reduce reliance on indwelling catheters. For example, a study in *JAMA Internal Medicine* found that avoiding catheters in postoperative patients reduced CAUTI rates by 54%.
Step 2: Implement Strict Aseptic Technique
When catheterization is necessary, adherence to sterile technique is non-negotiable. This includes hand hygiene, sterile gloves, and a sterile field for insertion. The catheter should be inserted using a closed drainage system to minimize bacterial entry. For instance, using a pre-packed, single-use catheter kit reduces contamination risk compared to open systems.
Step 3: Optimize Catheter Maintenance
Once in place, catheters require meticulous care. The drainage bag must be kept below bladder level to prevent backflow, and it should be emptied regularly without breaking the closed system. Patients and caregivers should be educated on avoiding kinks or dislodgment. For long-term catheter users, daily cleansing of the meatal area with antiseptic solutions (e.g., chlorhexidine) can reduce microbial colonization.
Caution: Avoid Overuse of Antibiotics
While antibiotics may seem like a preventive measure, their overuse can lead to antibiotic resistance and fungal infections. Prophylactic antibiotics are not recommended for routine catheterization. Instead, focus on removing the catheter as soon as clinically feasible, as duration of use is the strongest predictor of CAUTI risk.
Preventing CAUTIs requires a combination of judicious catheter use, rigorous aseptic technique, and proactive maintenance. By addressing each step in the catheterization process, healthcare teams can dramatically reduce infection rates, improve patient outcomes, and lower healthcare costs. For example, a bundled intervention at a large hospital system reduced CAUTI rates by 60% within one year, demonstrating the power of systematic prevention strategies.
Private vs. Public Hospitals: Key Differences and How to Choose Wisely
You may want to see also
Explore related products






![]()
Impact of catheter duration on UTI rates
Catheter-associated urinary tract infections (CAUTIs) account for approximately 75-80% of all hospital-acquired UTIs, making them a critical focus in healthcare settings. Among the various factors contributing to CAUTIs, the duration of catheterization stands out as one of the most significant. Research consistently shows that the risk of developing a UTI increases by 3-10% for every day a urinary catheter remains in place. This linear relationship underscores the importance of minimizing catheterization time whenever clinically feasible.
From an analytical perspective, the mechanism behind this increased risk is twofold. First, prolonged catheterization disrupts the natural urinary tract defenses, allowing bacteria to ascend more easily. Second, the catheter itself provides a surface for biofilm formation, which harbors pathogens and renders them resistant to antibiotics. Studies have demonstrated that after just 48 hours of catheterization, biofilm begins to develop, significantly elevating infection risk. This highlights the need for strict adherence to catheter insertion and removal protocols, particularly in high-risk populations such as elderly patients or those with compromised immune systems.
To mitigate the impact of catheter duration on UTI rates, healthcare providers should adopt evidence-based practices. For instance, implementing a daily assessment protocol to determine the necessity of continued catheterization can reduce unnecessary usage. Additionally, using catheter reminders or alerts in electronic health records can prompt timely removal. For patients requiring long-term catheterization, alternatives such as intermittent catheterization or the use of antimicrobial-coated catheters may be considered. However, these options must be weighed against individual patient needs and potential complications.
A comparative analysis of catheter duration across different clinical settings reveals striking disparities. In intensive care units, where catheters are often left in place for extended periods, CAUTI rates can exceed 20%. In contrast, surgical wards that prioritize early catheter removal report rates as low as 5%. This disparity emphasizes the role of institutional policies and clinician education in driving better outcomes. Hospitals that have successfully reduced CAUTI rates often cite interdisciplinary collaboration and data-driven quality improvement initiatives as key factors.
Practically speaking, reducing catheter duration requires a multifaceted approach. First, clinicians should ensure that catheters are inserted only when absolutely necessary, avoiding their use for convenience or non-indicated purposes. Second, clear guidelines for catheter removal should be established, with a focus on removing them within 24-48 hours whenever possible. Third, patient and caregiver education is essential, as informed individuals are more likely to question prolonged catheter use and advocate for alternatives. By addressing these areas, healthcare facilities can significantly decrease CAUTI rates and improve patient safety.
Understanding Abdominal Surgeries Requiring Extended Hospital Recovery Periods
You may want to see also
Explore related products






![]()
Antibiotic resistance in catheter-related UTIs
Catheter-associated urinary tract infections (CAUTIs) account for approximately 75-80% of all hospital-acquired UTIs, making them a leading cause of healthcare-associated infections. This staggering statistic underscores the critical need to address the growing challenge of antibiotic resistance in these cases. As catheters provide a direct pathway for bacterial colonization, the overuse and misuse of antibiotics in treating CAUTIs have accelerated the emergence of multidrug-resistant organisms, complicating patient care and increasing mortality rates.
Consider the mechanism: biofilms form on catheter surfaces within hours of insertion, shielding bacteria from antibiotics and the immune system. Common pathogens like *Escherichia coli* and *Klebsiella pneumoniae* thrive in these environments, often developing resistance to first-line agents such as ciprofloxacin and trimethoprim-sulfamethoxazole. For instance, extended-spectrum beta-lactamase (ESBL)-producing strains now require treatment with carbapenems, yet even these are threatened by the rise of carbapenem-resistant Enterobacterales (CRE). This resistance not only limits treatment options but also prolongs hospital stays, with some studies showing CAUTI-related costs exceeding $1,000 per patient.
To mitigate resistance, healthcare providers must adopt a multifaceted approach. First, prevention is paramount. Minimize catheter use to essential cases, ensure aseptic insertion, and remove catheters as soon as clinically feasible. For patients requiring long-term catheterization, consider alternatives like intermittent catheterization or condom catheters. Second, diagnostic precision is critical. Avoid empiric antibiotic treatment without confirming infection through urine culture and sensitivity testing. For example, a patient with asymptomatic bacteriuria (bacteria in urine without symptoms) should not receive antibiotics, as this practice fuels resistance without clinical benefit.
When treatment is necessary, tailor antibiotic regimens based on culture results and patient factors. For uncomplicated CAUTIs in adults, a 3- to 7-day course of nitrofurantoin (100 mg twice daily) or fosfomycin (3 g single dose) may suffice. In severe cases or immunocompromised patients, intravenous options like ceftriaxone (1 g daily) or ertapenem (1 g daily) might be required, but always de-escalate therapy once sensitivities are available. Caution is advised with fluoroquinolones due to rising resistance and potential adverse effects, particularly in older adults.
Finally, surveillance and education are essential. Hospitals should monitor CAUTI rates and antibiotic resistance patterns to guide empiric treatment protocols. Educate staff and patients on proper catheter care and the risks of antibiotic overuse. For example, a study in a U.S. hospital reduced CAUTI rates by 50% after implementing a bundle of interventions, including staff training and catheter removal protocols. By addressing antibiotic resistance in CAUTIs systematically, healthcare systems can preserve the efficacy of life-saving drugs while improving patient outcomes.
Do Hospitals Offer SI Clinics? Exploring Specialized Care Availability
You may want to see also
Frequently asked questions
Approximately 75-80% of hospital-acquired urinary tract infections (UTIs) are associated with the use of urinary catheters.
Catheter-associated UTIs are common because catheters provide a direct pathway for bacteria to enter the urinary tract, bypassing the body's natural defenses. Prolonged catheter use, improper insertion, and inadequate maintenance increase the risk of infection.
Hospitals can reduce catheter-related UTIs by implementing evidence-based practices such as using catheters only when necessary, ensuring proper insertion and maintenance, using sterile techniques, and promptly removing catheters when no longer needed. Staff education and adherence to infection control protocols are also critical.