Out-of-hospital cardiac arrest (OHCA) is a critical medical emergency with significant implications for public health, yet survival rates remain alarmingly low worldwide. Understanding the percentage of OHCA survival is crucial for evaluating the effectiveness of emergency response systems, bystander interventions, and medical treatments. Globally, the average survival rate for OHCA hovers around 10%, though this figure varies widely depending on factors such as location, response time, and the availability of defibrillators. In regions with robust emergency medical services and high bystander CPR rates, survival can reach up to 20-30%, highlighting the importance of community education and rapid intervention in improving outcomes. Despite advancements in resuscitation science, the low survival rates underscore the need for continued efforts to enhance prevention, response, and post-resuscitation care.
Explore related products






What You'll Learn
![]()
Survival rates by response time
Every minute counts in the event of an out-of-hospital cardiac arrest (OHCA). For every 60 seconds that pass without defibrillation, survival rates drop by 7-10%. This stark reality underscores the critical importance of response time in determining patient outcomes.
Studies consistently demonstrate a direct correlation between rapid response and increased survival. Data from the American Heart Association reveals that survival rates plummet from around 30-40% with a 1-minute response time to a mere 5% after 10 minutes. This dramatic decline highlights the narrow window of opportunity for successful resuscitation.
One key factor influencing response time is bystander intervention. Immediate CPR initiated by bystanders can double or even triple survival rates. Pairing CPR with the use of an automated external defibrillator (AED) within the first few minutes can further significantly improve outcomes. Public access to AEDs and widespread CPR training are therefore crucial in maximizing survival chances.
Consider the case of Seattle, a city renowned for its robust emergency response system. Their emphasis on rapid dispatch, widespread AED availability, and high bystander CPR rates have led to OHCA survival rates exceeding 60% – a testament to the power of swift action.
In contrast, rural areas often face significant challenges in achieving rapid response times due to greater distances and limited resources. Implementing innovative solutions like drone-delivered AEDs and community first responder programs can help bridge this gap and improve survival rates in these settings.
To maximize survival in OHCA, focus on these actionable steps:
- Learn CPR: Equip yourself with the skills to provide life-saving chest compressions.
- Know AED Locations: Familiarize yourself with the locations of AEDs in your community.
- Call 911 Immediately: Don't hesitate to call emergency services at the first sign of cardiac arrest.
- Advocate for Public Access AEDs: Support initiatives to increase the availability of AEDs in public spaces.
Remember, every second counts. By understanding the critical role of response time and taking proactive steps, we can all contribute to improving survival rates for those experiencing out-of-hospital cardiac arrest.
Where Was Ellen DeGeneres Born?
You may want to see also
Explore related products






![]()
Impact of bystander CPR on outcomes
Out-of-hospital cardiac arrest (OHCA) is a critical medical emergency with a survival rate that historically hovers around 10%, but this statistic masks a stark disparity: survival rates triple when bystanders perform cardiopulmonary resuscitation (CPR) before emergency services arrive. This intervention is not just beneficial—it’s transformative, turning a grim prognosis into a potentially survivable event.
Consider the mechanics of CPR: it maintains blood flow to vital organs, particularly the brain, during the critical minutes before defibrillation or advanced medical care. Without it, brain damage begins within 4–6 minutes, and death can follow within 10 minutes. Bystander CPR effectively buys time, acting as a bridge between collapse and professional intervention. Studies show that for every minute CPR is delayed, survival decreases by 7–10%. Conversely, immediate bystander CPR can double or even triple survival rates, particularly when combined with early defibrillation.
The impact of bystander CPR is not uniform across all OHCA cases. Its effectiveness varies by arrest location, witness status, and the presence of a shockable rhythm (ventricular fibrillation or pulseless ventricular tachycardia). For instance, in cases where bystanders initiate CPR and a defibrillator is used within 3–5 minutes, survival rates can soar to 50–70%. However, in rural areas or when CPR is not performed, survival rates plummet to single digits. Age and comorbidities also play a role, but the core principle remains: bystander CPR is a game-changer, regardless of the victim’s profile.
To maximize the impact of bystander CPR, focus on three actionable steps: first, recognize the signs of cardiac arrest (sudden collapse, no pulse, no breathing, or gasping). Second, call emergency services immediately and request a defibrillator. Third, begin hands-only CPR (chest compressions at a rate of 100–120 per minute) without delay. Training in CPR is invaluable, but even untrained bystanders can perform effective chest compressions. Public awareness campaigns, such as those in countries like Norway and Denmark, have demonstrated that increasing bystander CPR rates from 30% to 70% can elevate overall OHCA survival to 30–40%.
The takeaway is clear: bystander CPR is not just a good Samaritan act—it’s a critical determinant of survival in OHCA. Its impact is measurable, its execution accessible, and its potential to save lives undeniable. By empowering individuals to act swiftly and confidently, we can shift the survival curve upward, one compression at a time.
Pharmacists: Hospital Doctors or Not?
You may want to see also
Explore related products





![]()
Role of AED availability in survival
Out-of-hospital cardiac arrest (OHCA) survival rates remain alarmingly low, with global averages hovering around 10%. However, the presence of automated external defibrillators (AEDs) can dramatically shift this statistic. In communities where AEDs are widely available and accessible, survival rates can triple or even quadruple, reaching up to 40% in some cases. This stark contrast underscores the critical role AEDs play in bridging the gap between collapse and professional medical intervention.
Consider the chain of survival for OHCA: early recognition, immediate CPR, rapid defibrillation, and advanced care. AEDs directly address the third link, delivering a life-saving shock to restore a normal heart rhythm during ventricular fibrillation, the most common cause of OHCA. Unlike manual defibrillators, AEDs are designed for use by laypersons, providing voice prompts and visual instructions to guide bystanders through the process. For every minute defibrillation is delayed, survival decreases by 7–10%, making AED accessibility a literal race against time.
Deploying AEDs in public spaces—airports, gyms, schools, and offices—transforms these locations into potential lifelines. For instance, Japan’s strategic placement of AEDs in public areas has contributed to a 40% survival rate for witnessed OHCA, compared to 10% in the U.S., where AED availability is less widespread. Similarly, in Seattle, a city with robust AED programs, survival rates exceed 60% for shockable rhythms when bystanders use AEDs before emergency services arrive. These examples highlight the exponential impact of AED availability on survival outcomes.
However, simply placing AEDs in public spaces is insufficient. Effective AED programs require three critical components: visibility, maintenance, and public education. Devices must be clearly marked and regularly checked to ensure functionality. Equally important is training the public to recognize cardiac arrest and act swiftly. Programs like "CPR + AED" certification courses empower individuals to respond confidently, reducing hesitation and increasing the likelihood of timely intervention. Without these measures, even the most advanced AEDs remain underutilized tools.
In conclusion, AED availability is not just a factor in OHCA survival—it is a game-changer. By integrating AEDs into public infrastructure and fostering a culture of preparedness, communities can significantly improve survival rates. The evidence is clear: where AEDs are accessible and bystanders are trained, lives are saved. This simple yet powerful technology holds the key to transforming OHCA survival from a grim statistic to a story of hope and resilience.
Effective Strategies for Marketing Your Health Insurance Plan to Hospitals
You may want to see also
Explore related products






![]()
Survival differences by arrest location
Out-of-hospital cardiac arrest (OHCA) survival rates vary dramatically depending on where the event occurs, with location acting as a critical determinant of outcome. Arrests in public spaces, for instance, often benefit from bystander intervention, including CPR and AED use, which can double or triple survival odds. In contrast, residential settings, where 70% of OHCAs occur, frequently lack immediate access to trained responders, leading to lower survival rates—typically below 10%. This disparity underscores the importance of community CPR training and AED accessibility in homes and private areas.
Consider the workplace, where survival rates can reach up to 20% due to higher likelihoods of immediate CPR and AED availability. OSHA recommends that businesses with more than 10 employees have at least one trained first responder and an AED on-site. Schools and gyms, often equipped with AEDs and staff trained in emergency response, also report higher survival rates, approaching 30% in some studies. These environments demonstrate how preparedness directly correlates with improved outcomes, making them models for other settings.
In rural areas, survival rates plummet to as low as 5%, primarily due to prolonged response times and limited access to emergency services. Urban settings, on the other hand, see survival rates of up to 15%, thanks to faster EMS arrival times and denser populations of trained bystanders. A study in *Circulation* highlighted that every minute of delayed defibrillation reduces survival by 7–10%, emphasizing the need for decentralized emergency response systems in rural communities.
Practical steps can mitigate these location-based disparities. For residential settings, consider enrolling in CPR/AED certification courses, which are often available through local Red Cross chapters or hospitals. Advocate for AED installation in apartment complexes, gated communities, and private clubs. In rural areas, community-based initiatives like drone-delivered AEDs or volunteer first responder networks are emerging as innovative solutions. Urban planners and policymakers should prioritize AED placement in high-traffic areas and incentivize businesses to train employees in emergency response.
Ultimately, understanding survival differences by arrest location reveals actionable gaps in preparedness. By tailoring interventions to specific environments—whether through policy, technology, or education—we can significantly improve OHCA survival rates across all settings. The goal is clear: transform every location into a safer space for cardiac arrest response.
Unveiling the Key Supporters Behind American Women's Hospitals' Success
You may want to see also
Explore related products






![]()
Effect of age and health on survival rates
Out-of-hospital cardiac arrest (OHCA) survival rates are profoundly influenced by age and overall health, with younger, healthier individuals significantly outperforming older or chronically ill patients. Data from the American Heart Association reveals that survival to hospital discharge for OHCA ranges from 10% to 12% overall, but this drops to less than 5% in patients over 70. Age acts as a compounding risk factor, often intersecting with comorbidities like hypertension, diabetes, or heart disease, which further diminish survival odds. For instance, a 2020 study in *Circulation* found that patients under 65 with no pre-existing conditions had a 20% survival rate, compared to just 3% in those over 75 with multiple health issues.
Consider the physiological toll of aging on the cardiovascular system. Reduced myocardial elasticity, diminished coronary artery function, and slower response to resuscitation efforts all contribute to poorer outcomes in older adults. Healthier individuals, particularly those who maintain optimal blood pressure (below 120/80 mmHg), cholesterol levels (LDL < 100 mg/dL), and blood glucose (A1C < 5.7%), have a survival advantage. For example, a 55-year-old with a BMI of 24 and regular exercise habits is twice as likely to survive OHCA compared to a sedentary peer with uncontrolled hypertension. Practical steps like annual health screenings, adherence to prescribed medications, and lifestyle modifications can mitigate these risks, even in older populations.
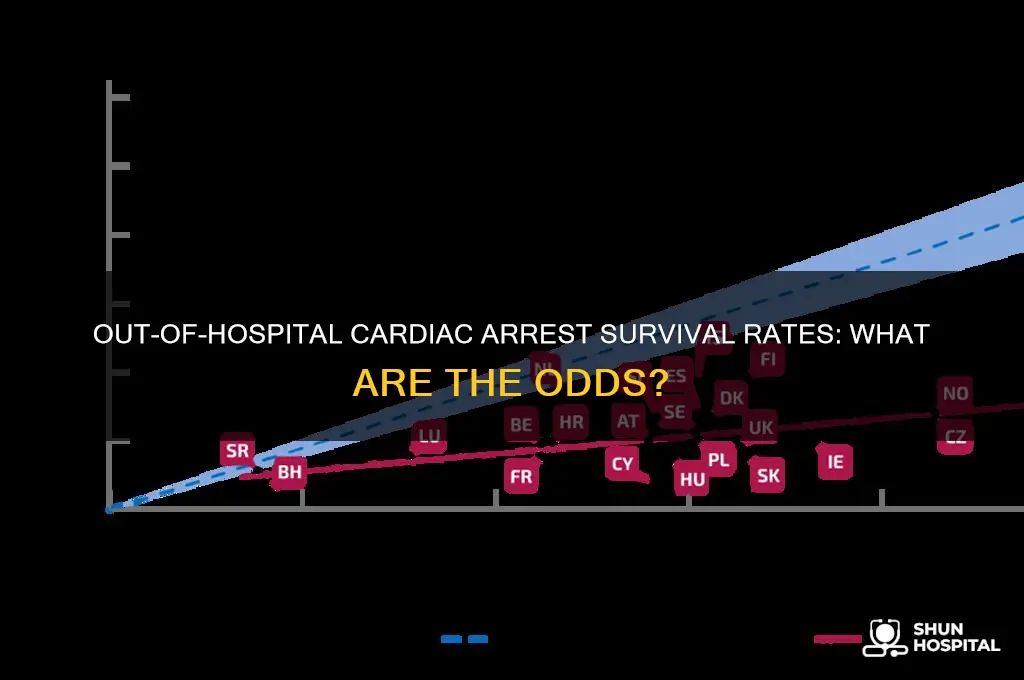
A comparative analysis of global OHCA data highlights the role of health systems in moderating age-related disparities. In Japan, where bystander CPR rates exceed 80% and public access to AEDs is widespread, survival rates for elderly patients are nearly double those in the U.S. This underscores the importance of community health initiatives, such as CPR training programs targeting older adults and their caregivers. Similarly, integrating wearable health monitors that detect arrhythmias early could improve outcomes in high-risk groups, though cost and accessibility remain barriers.
Persuasively, healthcare providers must prioritize age-specific interventions to improve OHCA survival. For younger patients, focus on preventing sudden cardiac arrest through genetic screening for conditions like hypertrophic cardiomyopathy. For older adults, emphasize multidisciplinary care plans that address polypharmacy, frailty, and social determinants of health. A 2021 *JAMA* study demonstrated that tailored post-resuscitation care, including therapeutic hypothermia and early coronary angiography, increased survival in patients over 65 by 15%. Such targeted strategies could redefine survival expectations across age groups.
Finally, a descriptive lens reveals the human impact of these disparities. Imagine a 45-year-old marathon runner who collapses during a race versus an 80-year-old with congestive heart failure at home. The former, with peak cardiovascular fitness and immediate bystander intervention, has a 70% chance of survival. The latter, despite optimal medical management, faces a 2% chance. This stark contrast illustrates why age and health must be central to OHCA research, policy, and practice. By addressing these factors head-on, we can transform survival from a statistical probability into a realistic expectation for all.
Accredited Hospitals: Wockhardt's NABH Excellence
You may want to see also
Frequently asked questions
The average survival rate for OHCA globally is approximately 10%, though this varies significantly by region and the quality of emergency response systems.
Bystander CPR can double or triple the survival rate of OHCA, increasing it to 20-30% in some cases, as it helps maintain blood flow until professional help arrives.
Approximately 50-70% of OHCA survivors have good neurological outcomes, meaning they recover without significant brain damage or disability.
Yes, younger patients generally have higher survival rates compared to older adults. For example, survival rates can be as high as 20-30% in younger age groups but drop to 5-10% in older populations.
The use of public access defibrillators (AEDs) can increase survival rates by up to 50-70% when used within the first few minutes of collapse, as they can restore a normal heart rhythm in cases of ventricular fibrillation.