Suicide in a hospital setting, though relatively rare compared to other locations, remains a significant concern due to the vulnerability of patients and the critical nature of healthcare environments. Studies suggest that approximately 1-2% of all suicides occur within hospitals, with higher rates observed in psychiatric wards and among patients with severe mental health conditions. Factors such as access to means, the stress of hospitalization, and underlying illnesses contribute to this risk. Understanding the prevalence and circumstances of hospital-based suicides is crucial for developing targeted prevention strategies and improving patient safety in healthcare settings.
Explore related products






What You'll Learn
- Global Hospital Suicide Rates: Overview of worldwide percentages of suicides occurring within hospital settings annually
- Mental Health Wards: Suicide rates specifically in psychiatric wards compared to general hospital areas
- Methods Used in Hospitals: Common methods of suicide attempted or completed within hospital environments
- Patient Demographics: Age, gender, and diagnosis profiles of individuals who commit suicide in hospitals
- Prevention Strategies: Effectiveness of hospital protocols and interventions in reducing suicide rates on premises
![]()
Global Hospital Suicide Rates: Overview of worldwide percentages of suicides occurring within hospital settings annually
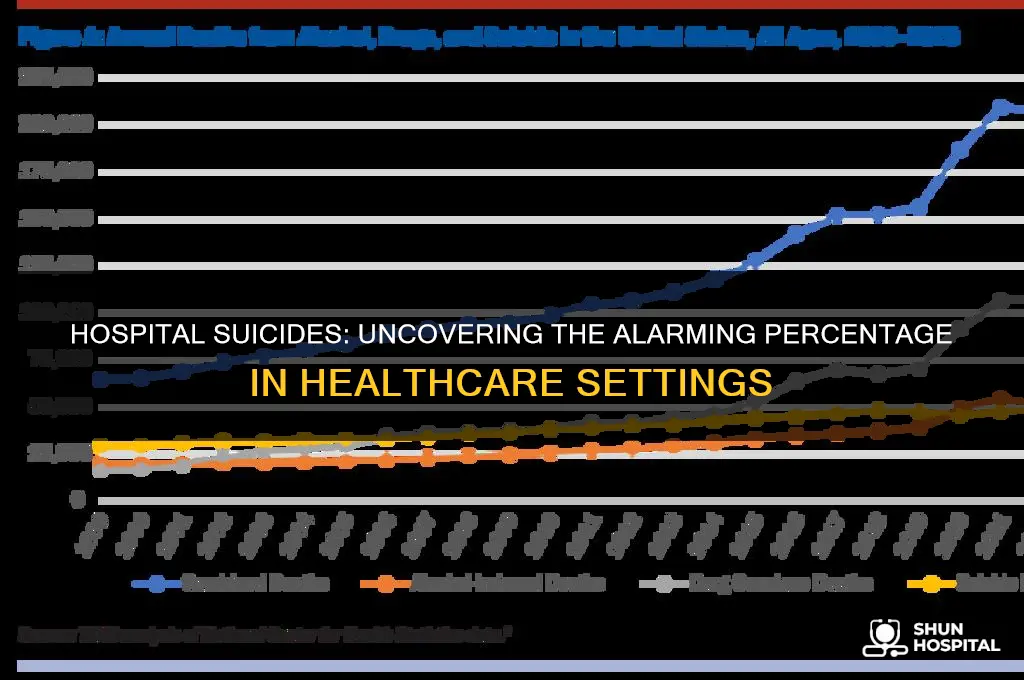
Hospital suicides, though a small fraction of global totals, reveal critical gaps in patient care and safety protocols. Data from the United States indicates that approximately 1-2% of suicides occur in hospital settings annually, with psychiatric wards accounting for the majority. In the UK, this figure rises to 3-5%, highlighting regional disparities in prevention strategies. These numbers underscore the paradox of hospitals—spaces designed for healing yet occasionally becoming sites of tragedy. Factors like understaffing, inadequate monitoring, and the vulnerability of patients in crisis contribute to these incidents, demanding urgent systemic reforms.
Analyzing global trends, low- and middle-income countries often report underestimates due to limited data collection and stigma surrounding mental health. For instance, studies in India suggest hospital suicides are underreported, with less than 1% documented despite anecdotal evidence of higher rates. In contrast, high-income nations like Sweden and Japan have invested in robust surveillance systems, revealing rates of 2-4% and emphasizing the role of cultural attitudes toward mental health care. These variations highlight the need for context-specific interventions, such as culturally sensitive training for healthcare staff and improved access to mental health resources.
A comparative study of hospital suicide rates across age groups reveals alarming patterns. Among adolescents and young adults, hospital suicides account for up to 10% of all suicides in some regions, often linked to inadequate crisis intervention and prolonged wait times for specialized care. For older adults, particularly those with chronic illnesses, the rate drops to 1-3%, but the lethality of methods (e.g., self-harm with medical equipment) increases. Tailored prevention strategies, such as age-specific risk assessments and enhanced monitoring for high-risk groups, could mitigate these disparities and save lives.
Persuasively, hospitals must adopt evidence-based practices to reduce suicide risks. Implementing the "Zero Suicide" framework, which emphasizes comprehensive screening, safety planning, and follow-up care, has shown promise in the U.S. and Australia. Similarly, environmental modifications—such as removing ligature points and securing access to medications—are cost-effective measures with proven impact. Policymakers and healthcare leaders must prioritize these initiatives, recognizing that even a single hospital suicide is one too many in an institution dedicated to preserving life.
Descriptively, the emotional toll of hospital suicides extends beyond statistics, affecting families, staff, and institutional reputations. Stories of patients who ended their lives in bathrooms or during unsupervised moments serve as stark reminders of the human cost of systemic failures. By fostering a culture of compassion, accountability, and continuous improvement, hospitals can transform from potential hazards into sanctuaries of hope and recovery for those in their most vulnerable moments.
When is Hospitalization Necessary for Pneumonia? Key Indicators Explained
You may want to see also
Explore related products


![The Hospital [DVD]](https://m.media-amazon.com/images/I/61oQ2sBPcmL._AC_UY218_.jpg)



![]()
Mental Health Wards: Suicide rates specifically in psychiatric wards compared to general hospital areas
Suicide rates within psychiatric wards present a paradox: these environments, designed for safety and treatment, still witness a significant proportion of hospital-based suicides. Studies indicate that while psychiatric wards account for only a small percentage of total hospital beds, they disproportionately contribute to in-hospital suicide statistics. A 2010 meta-analysis revealed that approximately 15-20% of all hospital suicides occur in psychiatric settings, despite these wards comprising less than 5% of hospital beds. This disparity underscores the unique challenges faced in mental health care environments.
The heightened risk in psychiatric wards can be attributed to several factors. Firstly, the patient population inherently includes individuals with severe mental health conditions, such as major depressive disorder, schizophrenia, and bipolar disorder, which are strongly associated with suicidal ideation. Secondly, the very nature of psychiatric care often involves managing patients during acute crises, when the risk of self-harm is at its peak. Despite stringent protocols, including regular observations and restricted access to harmful objects, the dynamic and unpredictable nature of mental illness can sometimes outpace preventive measures.
Comparatively, general hospital areas report lower suicide rates, though these incidents are not unheard of. In non-psychiatric settings, suicides often occur in patients admitted for physical health issues but who have underlying, undiagnosed, or untreated mental health conditions. A 2016 study found that approximately 5-10% of hospital suicides happen outside psychiatric wards, frequently in medical or surgical units. These cases highlight the need for comprehensive mental health screening across all hospital departments, as suicidal risk is not confined to psychiatric patients alone.
To address this issue, psychiatric wards must continually refine their risk assessment and management strategies. This includes enhancing staff training in suicide prevention, implementing evidence-based protocols, and fostering a therapeutic environment that balances safety with patient dignity. For general hospital areas, integrating mental health screenings into routine admissions and ensuring access to psychiatric consultation can help identify at-risk patients early. Ultimately, reducing hospital-based suicides requires a dual focus: strengthening specialized care in psychiatric wards and embedding mental health awareness throughout the entire healthcare system.
Writing a Hospital Volunteer Reference Letter: Tips and Best Practices
You may want to see also
Explore related products

![]()
Methods Used in Hospitals: Common methods of suicide attempted or completed within hospital environments
Hospitals, paradoxically, can become settings for suicide attempts despite their primary mission to heal. Understanding the methods employed within these environments is crucial for prevention. While hospitals implement stringent safety protocols, determined individuals exploit vulnerabilities in even the most controlled settings.
Common methods within hospitals often involve readily available resources. Patients may attempt self-strangulation using cords from medical equipment, bed linens, or even clothing. Access to medications presents another risk, with overdoses on painkillers, sedatives, or other pharmaceuticals being a significant concern. Inpatient units, particularly those treating mental health conditions, must be vigilant about securing potentially harmful items like sharps (needles, scissors) which could be used for self-harm.
The unique environment of hospitals also presents less conventional methods. Jumping from heights, such as windows or balconies, is a tragic reality, necessitating secure window locks and constant observation in high-risk cases. Patients might also attempt to use medical equipment itself as a weapon, manipulating IV poles or other devices for self-inflicted harm.
Even seemingly innocuous items can become tools for desperation. Plastic bags, for instance, have been used for suffocation attempts. This highlights the need for constant vigilance and a comprehensive approach to risk assessment that considers not only obvious dangers but also the potential misuse of everyday objects.
Preventing hospital suicides requires a multi-faceted approach. Beyond physical safeguards, it demands heightened staff awareness, thorough patient assessments, and a culture of open communication. Early identification of risk factors, coupled with appropriate interventions and support systems, are vital in mitigating the risk of suicide within the very places designed for healing.
Post-Hospital Isolation: Care Home Residents' Protocols Explained
You may want to see also
![]()
Patient Demographics: Age, gender, and diagnosis profiles of individuals who commit suicide in hospitals
Suicide in hospital settings is a critical yet under-discussed issue, with studies indicating that approximately 1-2% of all suicides occur in healthcare facilities. This statistic, though seemingly small, represents a significant challenge for patient safety and care quality. Understanding the demographics of those who take their lives in hospitals is essential for targeted prevention strategies. Age, gender, and diagnosis profiles emerge as key factors in identifying at-risk individuals.
Age plays a pivotal role in hospital-based suicides, with older adults being disproportionately represented. Research shows that individuals over 65 account for nearly 40% of in-hospital suicides, despite comprising a smaller percentage of the overall patient population. This vulnerability is often linked to chronic illnesses, social isolation, and a higher prevalence of depressive disorders in this age group. For instance, a study published in the *Journal of Gerontology* found that elderly patients with terminal diagnoses were three times more likely to attempt suicide during hospitalization. Hospitals must prioritize geriatric mental health screenings, particularly for those with prolonged stays or palliative care needs.
Gender disparities are equally striking, with men being more likely to complete suicide in hospitals than women. While women attempt suicide more frequently, men’s methods tend to be more lethal, a trend that persists in healthcare settings. A meta-analysis in *BMC Psychiatry* revealed that men accounted for 70% of hospital suicides, often using violent means such as self-strangulation or jumping from heights. This highlights the need for gender-specific interventions, such as closer monitoring of male patients, particularly those admitted for physical injuries or substance abuse, which are common risk factors.
Diagnosis profiles further refine the picture, with psychiatric and neurological conditions dominating the landscape. Patients admitted for depression, schizophrenia, or bipolar disorder are at the highest risk, contributing to over 50% of hospital suicides. However, non-psychiatric admissions also pose significant risks, especially for conditions like cancer, stroke, or chronic pain. For example, a study in *The Lancet* found that patients with a new cancer diagnosis were twice as likely to die by suicide during hospitalization compared to those without. Hospitals should implement multidisciplinary care teams that integrate mental health assessments into routine care, regardless of the primary diagnosis.
Practical steps can mitigate these risks. For older adults, regular mental health check-ins and family involvement can provide emotional support. For men, ensuring a safe environment by removing potential tools for self-harm is critical. For high-risk diagnoses, early psychiatric consultation and access to crisis intervention services can be lifesaving. By addressing these demographic-specific vulnerabilities, hospitals can transform from places of risk into sanctuaries of care.
Hospital vs. Family Clinic: Where Do Most Doctors Practice?
You may want to see also
![]()
Prevention Strategies: Effectiveness of hospital protocols and interventions in reducing suicide rates on premises
Hospitals, paradoxically, are not immune to suicide. While exact percentages vary by region and study, research suggests that between 1% and 5% of all suicides occur within healthcare settings, with inpatient psychiatric units bearing the brunt of this tragic statistic. This highlights a critical need for effective prevention strategies tailored to the unique vulnerabilities of hospitalized individuals.
Hospitals, tasked with healing, must confront the sobering reality of suicide within their walls.
Identifying High-Risk Individuals: The Foundation of Prevention
Effective prevention begins with meticulous screening and assessment. All patients, regardless of presenting complaint, should undergo a comprehensive suicide risk assessment upon admission. This should include a detailed psychiatric history, current mental state examination, and standardized screening tools like the Columbia-Suicide Severity Rating Scale (C-SSRS). Particularly vulnerable populations, such as those with a history of suicide attempts, severe depression, or substance abuse, require heightened vigilance and frequent re-evaluation.
Environmental Modifications: Creating a Safer Space
The physical environment plays a crucial role in suicide prevention. Hospitals should implement "ligature-resistant" designs, eliminating potential anchor points for hanging. This includes removing hooks, doorknobs, and pipes, and using break-away curtain rods and tamper-proof furniture. Regular safety audits are essential to identify and address potential hazards. Additionally, providing access to natural light, calming colors, and comfortable spaces can contribute to a less stressful environment, potentially reducing suicidal ideation.
Therapeutic Interventions: Addressing Underlying Distress
Beyond environmental modifications, evidence-based therapeutic interventions are vital. Cognitive-behavioral therapy (CBT) has proven effective in reducing suicidal thoughts and behaviors by helping individuals identify and challenge negative thought patterns. Dialectical behavior therapy (DBT), with its focus on emotion regulation and distress tolerance, is particularly beneficial for individuals with borderline personality disorder, a population at high risk for suicide. Pharmacotherapy, when used judiciously and under close monitoring, can also play a role in managing underlying mental health conditions contributing to suicidal risk.
Staff Training and Support: The Human Factor
The effectiveness of any prevention strategy hinges on the competence and compassion of hospital staff. All personnel, from nurses to custodial staff, should receive comprehensive training in suicide risk assessment, de-escalation techniques, and crisis intervention. This training should be ongoing, incorporating the latest research and best practices. Equally important is providing staff with adequate support to manage the emotional toll of working with suicidal patients. Access to supervision, debriefing sessions, and mental health services is crucial for preventing burnout and ensuring staff can provide the best possible care.
Continuous Evaluation and Improvement: A Dynamic Process
Suicide prevention in hospitals is not a static endeavor. Regular evaluation of protocols and interventions is essential to identify areas for improvement. This includes tracking suicide attempts and completions, analyzing near-miss incidents, and soliciting feedback from patients and staff. By embracing a culture of continuous learning and adaptation, hospitals can refine their prevention strategies, ultimately saving lives and fulfilling their mission of healing.
George Bush's Hospitalization: What We Know So Far
You may want to see also
Frequently asked questions
Approximately 1-2% of all suicides occur in a hospital setting, though rates can vary depending on the country and specific healthcare system.
Yes, suicides in hospitals are more common among patients with mental health disorders, those admitted for suicidal ideation, and individuals with chronic or terminal illnesses.
Hospitals implement prevention measures such as risk assessments, close monitoring, restricted access to lethal means, and specialized psychiatric care to reduce the risk of suicide.
Yes, suicides are more likely to occur in inpatient settings due to the higher concentration of at-risk patients and the opportunity for self-harm despite monitoring efforts.
Yes, the percentage varies globally due to differences in healthcare infrastructure, access to mental health services, and cultural attitudes toward suicide and hospitalization.