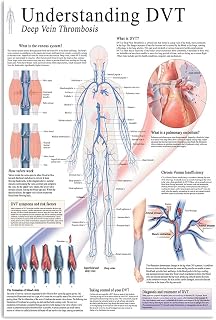
Deep vein thrombosis (DVT) is a serious and potentially life-threatening condition that can occur in hospitalized patients, particularly those who are immobilized or have undergone surgery. To prevent DVT, hospital management should implement a comprehensive strategy that includes risk assessment, early mobilization, and appropriate prophylaxis. This involves identifying high-risk patients through standardized screening tools, ensuring prompt administration of pharmacological prophylaxis such as anticoagulants when indicated, and promoting physical activity or compression devices to improve blood flow. Additionally, staff education and adherence to evidence-based guidelines are crucial to minimize the incidence of DVT and its complications, such as pulmonary embolism, ultimately enhancing patient safety and outcomes.
| Characteristics | Values |
|---|---|
| Risk Assessment | Conduct systematic DVT risk assessments for all hospitalized patients. |
| Prophylaxis Protocols | Implement evidence-based pharmacological (e.g., anticoagulants) and mechanical (e.g., compression devices) prophylaxis protocols. |
| Patient Education | Educate patients about DVT risks, symptoms, and preventive measures. |
| Staff Training | Train healthcare staff on DVT prevention guidelines and protocols. |
| Early Mobilization | Encourage early ambulation and mobility for at-risk patients. |
| Hydration Management | Ensure adequate hydration to maintain blood flow and reduce clot risk. |
| Regular Monitoring | Monitor patients regularly for signs of DVT or complications. |
| Use of Clinical Decision Tools | Utilize tools like PADUA or Caprini scores to stratify DVT risk. |
| Post-Discharge Planning | Provide clear discharge instructions for continued DVT prevention at home. |
| Audit and Feedback | Regularly audit compliance with DVT prevention protocols and provide feedback to staff. |
| Multidisciplinary Approach | Involve pharmacists, physiotherapists, and nurses in DVT prevention efforts. |
| Evidence-Based Updates | Stay updated with the latest guidelines (e.g., ACCP, NICE) and update protocols accordingly. |
| Documentation | Maintain accurate documentation of risk assessments and prophylaxis measures. |
| Resource Allocation | Ensure adequate resources (e.g., compression devices, anticoagulants) are available. |
| Patient-Specific Tailoring | Customize prophylaxis based on individual patient risk factors and comorbidities. |
Explore related products






What You'll Learn
- Early Risk Assessment: Screen patients on admission to identify DVT risk factors promptly
- Prophylaxis Protocols: Implement evidence-based anticoagulant and compression therapy guidelines for at-risk patients
- Mobility Promotion: Encourage early ambulation and exercise to improve blood flow in hospitalized patients
- Staff Education: Train healthcare staff on DVT prevention strategies and early symptom recognition
- Monitoring Compliance: Regularly audit and enforce adherence to DVT prevention protocols across departments
![]()
Early Risk Assessment: Screen patients on admission to identify DVT risk factors promptly
Deep vein thrombosis (DVT) is a silent threat, often manifesting without symptoms until it becomes life-threatening. Early risk assessment through systematic screening upon admission is the cornerstone of prevention. By identifying patients with predisposing factors—such as advanced age, obesity, recent surgery, prolonged immobility, or a history of thrombosis—hospitals can tailor preventive measures before complications arise. This proactive approach not only reduces morbidity and mortality but also minimizes healthcare costs associated with treating advanced DVT cases.
Consider the case of a 65-year-old post-surgical patient with a BMI of 35 and a family history of clotting disorders. Without screening, this patient might be overlooked until symptoms appear. However, a structured risk assessment tool, such as the Caprini score, can flag high-risk individuals like this one, prompting immediate interventions like anticoagulant therapy or compression devices. The Caprini score, for instance, assigns points based on factors like age (1 point for 41–60 years, 2 points for >60 years), surgery type (major procedures score 4 points), and comorbidities (active cancer scores 2 points). A total score of 5 or higher indicates moderate to high risk, necessitating intervention.
Screening must be seamless, integrated into the admission process without delaying care. Nurses or admitting physicians can administer brief questionnaires or checklists to identify risk factors. For example, asking about recent travel, prolonged bed rest, or hormonal therapy (e.g., oral contraceptives) takes less than 5 minutes but provides critical insights. Hospitals should standardize this process, ensuring all staff are trained to recognize and document risk factors accurately. Electronic health records (EHRs) can further streamline this by flagging high-risk patients automatically, triggering alerts for appropriate prophylaxis.
However, screening alone is insufficient without clear protocols for action. Hospitals must establish guidelines linking risk levels to interventions. For instance, low-risk patients might require only early ambulation and hydration, while high-risk patients may need low-molecular-weight heparin (LMWH) at a dose of 40 mg subcutaneously daily or intermittent pneumatic compression devices. These protocols should be evidence-based, regularly updated, and accessible to all clinical staff. Audits of compliance and outcomes can refine these protocols, ensuring they remain effective and adaptable to new research.
In conclusion, early risk assessment is not just a preventive measure—it’s a strategic imperative for hospitals aiming to curb DVT incidence. By embedding screening into admission workflows, leveraging validated tools, and linking risks to actionable interventions, hospitals can transform passive care into proactive protection. This approach not only safeguards patients but also reinforces a culture of vigilance and accountability in healthcare delivery.
Lone Peak Hospital: Is There a NICU?
You may want to see also
Explore related products






![]()
Prophylaxis Protocols: Implement evidence-based anticoagulant and compression therapy guidelines for at-risk patients
Deep vein thrombosis (DVT) is a significant concern in hospitalized patients, with potentially life-threatening consequences if left untreated. Implementing evidence-based prophylaxis protocols is crucial to mitigating this risk. Hospital management must prioritize the development and enforcement of guidelines that combine anticoagulant therapy and compression methods, tailored to individual patient needs.
Evidence-based Anticoagulant Therapy:
For surgical patients, low molecular weight heparin (LMWH) or unfractionated heparin (UFH) is often recommended, with dosing adjusted for age, weight, and renal function. For instance, enoxaparin 40 mg subcutaneously once daily is a common prophylactic dose for general surgery patients, while higher-risk cases may require 30 mg every 12 hours. Non-surgical patients might benefit from direct oral anticoagulants (DOACs) like rivaroxaban 10 mg daily, provided there are no contraindications. It’s essential to assess bleeding risks and monitor renal function, especially in elderly patients over 75, who may require dose reductions.
Compression Therapy Guidelines:
Mechanical prophylaxis, such as graduated compression stockings (GCS) or intermittent pneumatic compression (IPC) devices, should complement pharmacological measures, particularly in patients with contraindications to anticoagulants. GCS should provide a minimum pressure of 18 mmHg at the ankle, with proper fitting to ensure efficacy. IPC devices, which inflate and deflate to mimic ambulation, are particularly effective in post-surgical and immobilized patients. Staff should be trained to apply these devices correctly, ensuring coverage of the calf and thigh, and to inspect the skin daily for signs of irritation or pressure injury.
Tailoring Protocols to At-Risk Populations:
Certain patient groups, such as those with a history of thrombosis, obesity, or prolonged immobilization, require intensified prophylaxis. For example, bariatric patients may need higher doses of LMWH (e.g., enoxaparin 40 mg twice daily) or extended duration of therapy. Pregnant patients, who are at increased risk due to hypercoagulability, should receive prophylactic LMWH rather than DOACs, which are contraindicated during pregnancy. Pediatric patients require weight-based dosing, with careful monitoring to avoid overdosing.
Practical Implementation and Monitoring:
Hospitals should integrate prophylaxis protocols into electronic health records (EHRs) to ensure consistent application. Automated alerts can remind clinicians to assess DVT risk upon admission and initiate appropriate measures. Regular audits of compliance and outcomes are essential to identify gaps and refine protocols. For instance, tracking rates of DVT, pulmonary embolism, and bleeding complications can highlight areas for improvement. Staff education is critical; nurses and physicians must understand the rationale behind each intervention and how to troubleshoot issues, such as patient discomfort with compression devices or missed anticoagulant doses.
By adopting a structured, evidence-based approach to prophylaxis, hospital management can significantly reduce the incidence of DVT, improving patient safety and outcomes. This requires not only clear guidelines but also ongoing evaluation and adaptation to emerging research and clinical experience.
Does SL Lukes Hospital TV Broadcast Astros Baseball Games?
You may want to see also
Explore related products






![]()
Mobility Promotion: Encourage early ambulation and exercise to improve blood flow in hospitalized patients
Prolonged immobility is a significant risk factor for deep vein thrombosis (DVT) in hospitalized patients, as stagnant blood flow increases the likelihood of clot formation. Hospital management can mitigate this risk by implementing mobility promotion programs that encourage early ambulation and exercise. Such initiatives not only enhance blood circulation but also improve overall patient recovery and satisfaction.
Steps to Implement Mobility Promotion:
- Assess Patient Mobility Levels: Upon admission, evaluate each patient’s ability to move independently, considering factors like age, comorbidities, and surgical status. Tailor mobility plans accordingly, ensuring safety and feasibility.
- Set Clear Ambulation Goals: For low-risk patients, aim for 3–5 minutes of walking every hour during waking hours. Post-surgical patients may start with shorter intervals (e.g., 1–2 minutes every 2 hours) and gradually increase duration.
- Incorporate In-Bed Exercises: For bedridden patients, introduce simple exercises like ankle pumps, leg raises, or thigh squeezes, performed 10–15 times every 2–3 hours to stimulate blood flow.
- Use Mobility Aids: Provide walkers, canes, or assistive devices as needed, ensuring proper training for both patients and staff.
- Educate Patients and Families: Teach patients the importance of movement in preventing DVT and involve family members in encouraging mobility during visits.
Cautions and Considerations:
While mobility promotion is beneficial, it must be balanced with patient safety. Avoid overexertion, especially in elderly or frail patients, and monitor for signs of dizziness, pain, or fatigue. Post-surgical patients should follow surgeon-approved protocols to prevent complications. Additionally, ensure adequate staffing to supervise mobility activities, particularly in high-risk units like intensive care.
Practical Tips for Success:
- Use visual aids like posters or infographics to remind patients and staff about mobility goals.
- Schedule mobility sessions around medication or meal times to integrate them seamlessly into daily routines.
- Leverage technology, such as wearable activity trackers or mobile apps, to monitor progress and motivate patients.
By prioritizing early ambulation and exercise, hospital management can significantly reduce the incidence of DVT while fostering a culture of proactive patient care. This approach not only addresses a critical clinical need but also enhances the overall quality of hospital stays.
Understanding the Step-Down Unit: A Transitional Care Ward in Hospitals
You may want to see also
Explore related products





![]()
Staff Education: Train healthcare staff on DVT prevention strategies and early symptom recognition
Healthcare professionals are often the first line of defense against deep vein thrombosis (DVT), yet many lack comprehensive training in its prevention and early detection. This knowledge gap can lead to delayed interventions, increasing the risk of life-threatening complications like pulmonary embolism. To address this, hospital management must prioritize staff education, ensuring every team member, from nurses to physicians, is equipped with the latest evidence-based strategies.
Begin by implementing structured training programs that cover the fundamentals of DVT prevention, including risk assessment tools such as the Caprini score. Staff should learn to identify high-risk patients—those over 60, post-surgical cases, or individuals with a history of thrombosis—and tailor interventions accordingly. For instance, teaching nurses to administer low-molecular-weight heparin (LMWH) at the correct dosage (e.g., 40 mg enoxaparin daily for medical patients) can significantly reduce DVT incidence. Practical demonstrations of proper compression stocking application and graduated pressure device usage should also be included, as improper techniques can render these tools ineffective.
Early symptom recognition is equally critical. Train staff to detect subtle signs like calf tenderness, unilateral leg swelling, or unexplained shortness of breath, which may precede more obvious symptoms. Role-playing scenarios can help clinicians practice responding to these red flags, ensuring swift action. For example, a nurse noticing persistent leg pain in a post-operative patient should immediately escalate to a physician for further evaluation, potentially including a D-dimer test or ultrasound.
However, education alone is insufficient without ongoing reinforcement. Regular refresher sessions, coupled with accessible resources like quick-reference guides or digital modules, can help maintain competency. Hospitals should also track staff performance through audits or case reviews, identifying areas for improvement. For instance, if audits reveal delays in LMWH administration, targeted training on medication protocols can be provided.
By investing in staff education, hospital management not only enhances patient safety but also fosters a culture of proactive care. Empowering healthcare professionals with the knowledge and skills to prevent and recognize DVT transforms them into vigilant advocates, reducing morbidity and mortality while improving overall care quality. This strategic focus on education is a cornerstone of effective DVT prevention in any healthcare setting.
Your Right to Leave the Hospital
You may want to see also
Explore related products






![]()
Monitoring Compliance: Regularly audit and enforce adherence to DVT prevention protocols across departments
Hospitals must treat DVT prevention protocols as non-negotiable standards, not suggestions. Regular audits are the backbone of this enforcement, ensuring every department—from surgery to geriatrics—adheres strictly to evidence-based practices. For instance, a quarterly audit might reveal that the orthopedics unit consistently underutilizes sequential compression devices (SCDs) post-surgery, while the ICU over-relies on unfractionated heparin without proper monitoring. These discrepancies highlight systemic gaps that audits bring to light, allowing management to intervene before complications arise.
Consider the audit process itself: it should be structured yet adaptable. Begin with a checklist tailored to each department’s risk profile. For high-risk surgical units, verify that mechanical prophylaxis (e.g., SCDs) is initiated within 6 hours of surgery and that pharmacological prophylaxis (e.g., low-molecular-weight heparin 40 mg subcutaneously daily) is administered as per protocol. In contrast, audits in medical wards should focus on timely risk assessments using tools like the Padua score, ensuring patients with scores ≥4 receive appropriate prophylaxis. Cross-referencing patient charts with pharmacy records can uncover discrepancies, such as missed doses or inappropriate dosing in elderly patients (e.g., reduced enoxaparin doses for those with creatinine clearance <30 mL/min).
Enforcement requires more than identifying lapses—it demands accountability and education. When audits reveal non-compliance, address root causes rather than assigning blame. For example, if nurses in the neurology ward skip DVT assessments due to time constraints, management might introduce streamlined documentation tools or allocate additional staff during peak hours. Simultaneously, provide ongoing training to address knowledge gaps, such as clarifying when to use graduated compression stockings (GCS) versus SCDs. Incentivizing compliance through recognition programs or linking adherence rates to departmental performance metrics can further motivate staff.
A comparative analysis of audit data across departments can reveal systemic trends. If multiple units struggle with pharmacological prophylaxis timing, the issue may lie in pharmacy dispensing delays or unclear order sets. Hospitals might then standardize order sets to include default prophylaxis protocols, reducing variability. For instance, a hospital in Canada reduced DVT rates by 30% after implementing a system-wide protocol that mandated automatic pharmacological prophylaxis orders for all surgical patients unless contraindicated. Such data-driven interventions demonstrate how audits can catalyze hospital-wide improvements.
Finally, transparency is key. Share audit findings with all staff, not just department heads, to foster a culture of collective responsibility. Visual aids, such as compliance dashboards displayed in staff areas, can make progress tangible. For example, a color-coded chart showing SCD usage rates across units might inspire friendly competition. Pair this with regular feedback sessions where staff can suggest protocol refinements based on their experiences. By treating compliance monitoring as an iterative, collaborative process, hospitals can transform DVT prevention from a checkbox exercise into a cornerstone of patient safety.
Who Took Tyre Nichols to Hospital?
You may want to see also
Frequently asked questions
Hospital management should ensure all patients are screened for DVT risk using validated tools (e.g., PADUA or Caprini score) upon admission and periodically during their stay. This assessment should consider factors like age, mobility, surgery type, and medical history to guide appropriate prophylaxis.
Management should develop and enforce evidence-based protocols for DVT prophylaxis, including mechanical (e.g., compression devices) and pharmacological (e.g., anticoagulants) interventions. Regular staff training, audits, and reminders can improve adherence to these protocols.
Management should support initiatives that encourage early and frequent patient mobility, such as providing adequate staffing, creating mobility protocols, and educating patients and families about the importance of movement in DVT prevention.
Management should establish a system for tracking DVT incidence, prophylaxis compliance, and patient outcomes. Regular reviews, feedback loops, and quality improvement initiatives can help identify gaps and optimize prevention strategies.