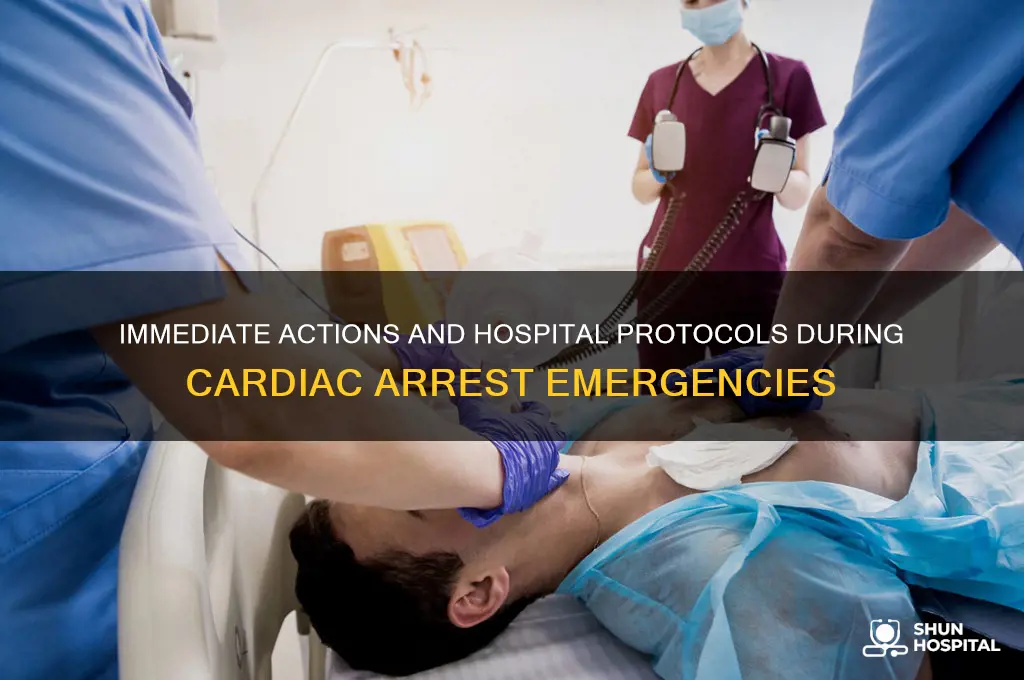
During a cardiac arrest in a hospital setting, immediate and coordinated action is crucial to maximize the chances of survival. The first step is to activate the hospital’s emergency response system by calling a code blue, which alerts a rapid response team, including doctors, nurses, and resuscitation specialists. Simultaneously, cardiopulmonary resuscitation (CPR) should be initiated without delay, maintaining consistent chest compressions at a rate of 100-120 per minute. Defibrillation should be performed as soon as possible if a shockable rhythm (ventricular fibrillation or pulseless ventricular tachycardia) is detected. The team must also establish intravenous access, administer adrenaline (epinephrine) as per advanced life support (ALS) protocols, and address reversible causes of cardiac arrest (e.g., hypoxia, hypovolemia, hypo/hyperkalemia, hypothermia, thrombosis, or tamponade). Continuous monitoring of the patient’s rhythm and vital signs is essential, and post-resuscitation care, including targeted temperature management and critical care support, should be initiated promptly to optimize outcomes.
| Characteristics | Values |
|---|---|
| Immediate Recognition | Recognize signs of cardiac arrest (unresponsiveness, no normal breathing). |
| Activate Emergency Response | Call for help (e.g., "Code Blue" in hospitals) and notify the team. |
| Start CPR | Begin high-quality chest compressions (depth: 2-2.4 inches, rate: 100-120/min). |
| Defibrillation | Use an AED or defibrillator if ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT) is detected. |
| Airway Management | Secure airway with bag-mask ventilation or advanced airway (e.g., endotracheal tube). |
| Medications | Administer adrenaline (epinephrine) every 3-5 minutes, amiodarone for shock-refractory VF/VT. |
| Team Communication | Assign roles (compressions, airway, medications, monitoring) for coordinated care. |
| Rhythm Monitoring | Continuously monitor heart rhythm to guide defibrillation and treatment. |
| Post-Resuscitation Care | Initiate targeted temperature management (32-36°C) and assess for ROSC (return of spontaneous circulation). |
| Documentation | Record time of collapse, interventions, and outcomes for quality review. |
| Family Communication | Update family members promptly and provide emotional support. |
| Ethical Considerations | Discuss goals of care and potential limitations with the patient's family. |
| Quality Improvement | Review the case for adherence to guidelines and identify areas for improvement. |
Explore related products






What You'll Learn
- Immediate CPR: Start chest compressions at 100-120/min, depth 2-2.4 inches; ensure minimal interruptions
- Defibrillation: Use AED promptly; deliver shock for shockable rhythms (VF/VT), then resume CPR
- Airway Management: Secure airway with bag-mask or advanced airway (e.g., intubation) if trained
- Medications: Administer epinephrine every 3-5 minutes; consider antiarrhythmics for shock-refractory VF/VT
- Team Communication: Assign roles clearly (compressions, airway, meds, monitoring) for coordinated resuscitation
![]()
Immediate CPR: Start chest compressions at 100-120/min, depth 2-2.4 inches; ensure minimal interruptions
During a cardiac arrest in a hospital setting, immediate CPR is critical to maintaining blood flow and oxygen to vital organs. The first step is to start chest compressions without delay, as every second counts. The recommended rate for chest compressions is 100 to 120 compressions per minute, which ensures adequate circulation. This pace is roughly equivalent to the beat of the song "Stayin' Alive" by the Bee Gees, which can serve as a mental metronome for rescuers. It is essential to maintain this rate consistently to maximize the effectiveness of CPR.
The depth of chest compressions is equally important and should be 2 to 2.4 inches (5 to 6 cm) for adults. Compressing the chest to this depth allows for sufficient blood flow to the heart and brain. To achieve this, place the heel of one hand on the center of the chest (over the lower half of the sternum) and use your body weight to push straight down. Allow the chest to fully recoil between compressions, as this recoil is crucial for venous return and effective blood circulation. Avoid leaning on the chest during the recoil phase, as it can reduce the efficiency of the compressions.
Minimizing interruptions in chest compressions is a key principle in high-quality CPR. Research shows that interruptions longer than 10 seconds can significantly decrease the chances of survival. To ensure minimal interruptions, coordinate with the team to perform tasks efficiently. For example, if a defibrillator is being prepared, continue compressions until the shock is ready to deliver. Similarly, during airway management or medication administration, assign a team member to take over compressions briefly to maintain continuous chest compressions. The goal is to keep interruptions under 10 seconds and resume compressions immediately afterward.
In a hospital setting, team communication is vital to maintaining uninterrupted CPR. Clearly assign roles and responsibilities to each team member, such as one person performing compressions, another preparing the defibrillator, and a third managing the airway. Use clear, concise communication to coordinate actions and avoid confusion. For instance, announce when compressions are paused and when they should resume. Effective teamwork ensures that chest compressions are delivered consistently and that interruptions are kept to an absolute minimum.
Finally, monitor the quality of chest compressions throughout the resuscitation effort. Many hospitals have feedback devices that can provide real-time data on compression rate, depth, and recoil. Utilize these tools to ensure that compressions meet the recommended guidelines. If manual feedback is necessary, assign a team member to observe and provide corrections as needed. High-quality chest compressions at the correct rate and depth, with minimal interruptions, significantly improve the chances of a successful outcome during cardiac arrest in a hospital setting.
The Role of a Ward Sister in Hospitals
You may want to see also
Explore related products

$9.99 $18.95



$35 $49.99


![]()
Defibrillation: Use AED promptly; deliver shock for shockable rhythms (VF/VT), then resume CPR
During a cardiac arrest in a hospital setting, defibrillation is a critical intervention that can significantly improve survival rates, especially when performed promptly. The first step is to use an Automated External Defibrillator (AED) immediately upon recognition of a cardiac arrest. AEDs are designed to analyze the patient’s heart rhythm and determine if a shock is needed. In the hospital, ensure the AED is readily accessible and activated as soon as possible, as time is of the essence. The device will provide clear voice prompts to guide the responder through the process, ensuring even those with minimal training can operate it effectively.
Once the AED is applied, it will analyze the heart rhythm to identify whether the patient is in a shockable rhythm, specifically ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT). These rhythms are chaotic and ineffective in pumping blood, and they require an electrical shock to restore a normal heartbeat. If the AED advises a shock, ensure all team members are clear of the patient, deliver the shock as instructed, and then immediately resume CPR without delay. The shock itself does not restart the heart but momentarily stops it, allowing the heart’s natural pacemaker to regain control. CPR should continue for approximately 2 minutes (or 5 cycles of compressions and ventilations) before the AED reanalyzes the rhythm.
It is crucial to minimize pauses in chest compressions during the defibrillation process. After delivering a shock, resume CPR immediately, as this maintains blood flow to vital organs. The AED will prompt another rhythm analysis after the CPR cycle, and if a shock is still indicated, the process is repeated. Avoid excessive delays in pad placement or rhythm analysis, as prolonged downtime reduces the chances of successful defibrillation. Coordination among the healthcare team is essential to ensure seamless transitions between shocking and CPR.
In a hospital setting, manual defibrillators may also be used by trained personnel, offering more control over the shock delivery process. However, the principles remain the same: identify shockable rhythms, deliver the shock, and resume CPR promptly. The goal is to restore a perfusing rhythm as quickly as possible while maintaining adequate circulation through uninterrupted CPR. Effective communication and adherence to the AED’s prompts are key to successful defibrillation and improving patient outcomes during cardiac arrest.
Finally, remember that defibrillation is just one component of the overall cardiac arrest response. It must be integrated with high-quality CPR, airway management, and medication administration as part of the ACLS (Advanced Cardiac Life Support) protocol. Regular training and drills in the hospital setting can ensure that all staff members are prepared to act swiftly and confidently during a cardiac arrest, maximizing the chances of survival for the patient.
Hospital Heroes: Who Wheels the Gurney?
You may want to see also
Explore related products






![]()
Airway Management: Secure airway with bag-mask or advanced airway (e.g., intubation) if trained
During a cardiac arrest in a hospital setting, airway management is a critical priority to ensure adequate oxygenation and ventilation. The first step is to assess the patient’s airway for any obstructions, such as vomit, blood, or foreign objects. If the airway is clear, immediately secure it using a bag-mask device. This involves placing a mask over the patient’s nose and mouth, creating a seal, and manually squeezing the bag to deliver oxygenated air. Ensure the head is properly positioned using the head-tilt chin-lift maneuver to open the airway. A second rescuer should simultaneously provide chest compressions to maintain circulation. The bag-mask technique is effective and should be initiated promptly by trained personnel.
If the patient’s condition deteriorates or if the rescuer is trained in advanced airway techniques, consider inserting an advanced airway device, such as an endotracheal tube (intubation). Intubation provides a more secure airway and reduces the risk of aspiration, but it requires skill and should only be attempted by trained providers. Before proceeding, pre-oxygenate the patient with 100% oxygen via bag-mask for at least 3 breaths to maximize oxygen reserves. Use direct laryngoscopy or a video laryngoscope to visualize the vocal cords and insert the tube. Confirm proper tube placement by observing chest rise, listening for bilateral breath sounds, and using a capnography monitor to detect CO2.
In situations where intubation is not feasible or fails, consider alternative advanced airway options such as a laryngeal mask airway (LMA). An LMA is easier to insert and can provide adequate ventilation while minimizing interruptions to chest compressions. Place the LMA into the hypopharynx to create a seal, and connect it to the bag-mask or ventilator. Ensure proper positioning by checking for adequate chest rise and the absence of air leakage. Regardless of the method chosen, continuous monitoring of oxygen saturation and end-tidal CO2 is essential to guide management.
Throughout airway management, minimize interruptions to chest compressions, as these are vital for maintaining perfusion to the heart and brain. Assign a team member to coordinate efforts and ensure seamless transitions between airway interventions and other resuscitative measures. Communicate clearly and use a structured approach, such as the ABC (Airway, Breathing, Circulation) framework, to maintain focus and efficiency. Remember, the goal is to restore spontaneous circulation while preventing hypoxic brain injury, and effective airway management plays a pivotal role in achieving this.
Finally, document all airway interventions, including the method used, timing, and any complications encountered. This information is crucial for ongoing care and quality improvement. After securing the airway, focus on other aspects of the resuscitation, such as defibrillation, administration of medications, and monitoring vital signs. Continuous training and simulation exercises are essential to ensure all team members are proficient in airway management techniques and can respond confidently during a cardiac arrest.
Cal Poly Animal Hospital: What's the Deal?
You may want to see also
Explore related products






![]()
Medications: Administer epinephrine every 3-5 minutes; consider antiarrhythmics for shock-refractory VF/VT
During a cardiac arrest in a hospital setting, the administration of medications plays a critical role in the resuscitation process. One of the cornerstone medications is epinephrine, which should be administered every 3 to 5 minutes. Epinephrine acts as a vasoconstrictor and increases coronary and cerebral perfusion, thereby improving the chances of restoring spontaneous circulation (ROSC). The first dose of epinephrine should be given as soon as feasible after the onset of cardiac arrest if defibrillation is not immediately successful or if the rhythm is non-shockable (e.g., asystole or pulseless electrical activity). Subsequent doses should be repeated every 3 to 5 minutes to maintain adequate perfusion pressure. It is essential to ensure that epinephrine is administered intravenously, as this route provides the most rapid and reliable effect.
In addition to epinephrine, antiarrhythmic medications should be considered for patients with shock-refractory ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT). These rhythms are often resistant to defibrillation alone, and pharmacological intervention can be life-saving. Amiodarone is the first-line antiarrhythmic agent recommended in this scenario. A 300 mg bolus should be administered intravenously after the third shock for VF/VT, with a second dose of 150 mg considered if the initial dose is ineffective. Alternatively, lidocaine can be used, although it is generally considered less effective than amiodarone. The choice of antiarrhythmic should be guided by the patient’s clinical status and the availability of the medication.
It is crucial to monitor the patient closely after administering antiarrhythmics, as these medications can have significant side effects, including hypotension and prolongation of the QT interval. Continuous electrocardiographic monitoring is essential to detect any adverse effects promptly. Additionally, antiarrhythmics should not delay defibrillation attempts, as electrical therapy remains the primary treatment for VF/VT. The combination of timely defibrillation and appropriate antiarrhythmic use can significantly improve the likelihood of successful resuscitation.
When administering these medications, the healthcare team must ensure clear communication and coordination. The timing of each dose should be documented accurately to avoid errors or omissions. In cases where intravenous access is challenging, intraosseous administration of epinephrine and antiarrhythmics is a viable alternative, as it provides rapid drug delivery to the systemic circulation. The goal is to maintain a structured and systematic approach to medication administration while simultaneously performing high-quality chest compressions and managing the airway.
Finally, it is important to reassess the patient’s rhythm and hemodynamic status after each intervention. If ROSC is not achieved despite multiple doses of epinephrine and antiarrhythmics, the team should consider other potential causes of cardiac arrest, such as hypovolemia, hypoxia, acidosis, or hypothermia, and address these issues as part of the comprehensive resuscitation effort. The use of medications during cardiac arrest must be integrated into a broader, multidisciplinary approach to maximize the chances of a successful outcome.
Parking Tips for Visitors at Nationwide Children's Hospital: A Guide
You may want to see also
Explore related products





![]()
Team Communication: Assign roles clearly (compressions, airway, meds, monitoring) for coordinated resuscitation
During a cardiac arrest in a hospital setting, effective team communication is paramount to ensure a coordinated and efficient resuscitation effort. The first step is to assign roles clearly to each team member, ensuring everyone knows their specific responsibilities. The core roles typically include compressions, airway management, medications, and monitoring. The team leader should immediately designate these roles based on the expertise and availability of the team members. For instance, the most experienced provider should take on the role of managing the airway, while a skilled nurse or physician should handle medication administration. Clear role assignment minimizes confusion and ensures that critical tasks are performed without delay.
The compressions role is vital, as high-quality chest compressions are the cornerstone of resuscitation. The assigned team member should focus solely on delivering consistent, uninterrupted compressions at the correct rate and depth. They should also be prepared to rotate with another team member every two minutes to avoid fatigue and maintain compression quality. The team leader must communicate clearly when rotations are needed to ensure seamless transitions. Effective communication here ensures that compressions are never paused unnecessarily, maintaining perfusion to vital organs.
Airway management is another critical role that requires clear communication. The assigned team member should focus on securing the airway, whether through bag-mask ventilation, endotracheal intubation, or other advanced techniques. They must communicate their actions and any challenges encountered, such as difficulty ventilating or intubating. The team leader should be informed immediately if advanced airway placement is unsuccessful, as alternative strategies may need to be implemented promptly. Clear communication ensures that the team can adapt quickly to maintain adequate oxygenation and ventilation.
The medications role involves administering lifesaving drugs such as epinephrine, amiodarone, or bicarbonate as per the resuscitation protocol. The assigned team member must communicate verbally each medication given, including the dose and time of administration, to ensure accurate documentation and prevent errors. They should also anticipate the need for subsequent doses and prepare them in advance. The team leader should confirm receipt of this information to ensure everyone is aware of the patient’s treatment progression. This level of communication is essential for maintaining a coordinated and evidence-based approach to care.
Finally, the monitoring role involves tracking the patient’s vital signs, ECG rhythm, and response to interventions. The assigned team member should provide continuous updates to the team, such as changes in heart rhythm or the return of spontaneous circulation (ROSC). Clear and concise communication from the monitor ensures that the team leader can make informed decisions about the next steps in resuscitation. For example, if a shockable rhythm is identified, the monitor must communicate this immediately so that defibrillation can be performed without delay. Effective communication in this role keeps the entire team aligned and focused on the shared goal of restoring life.
In summary, assigning roles clearly for compressions, airway, meds, and monitoring is essential for coordinated resuscitation during a cardiac arrest in a hospital. Each team member must understand their responsibilities and communicate effectively to ensure seamless execution of tasks. The team leader plays a critical role in facilitating this communication, ensuring that everyone is informed and aligned. By prioritizing clear role assignment and open dialogue, the team can maximize their efficiency and improve the patient’s chances of survival.
Hospital NCPs: Who Are They and What Do They Do?
You may want to see also
Frequently asked questions
Immediately activate the hospital’s emergency response system by calling for help or pressing the emergency button. Begin CPR if trained, starting with chest compressions at a rate of 100-120 per minute. Use an AED (automated external defibrillator) if available, following its voice prompts.
The hospital team follows a standardized protocol, often called a "code blue." This includes rapid assessment, defibrillation if needed, administration of medications, and advanced airway management. The team works collaboratively to restore the patient’s heart rhythm and stabilize their condition.
Bystanders should alert nearby staff or call for help immediately. If trained and no one else is available, they should start CPR and use an AED if accessible. Clear the area for medical professionals and follow their instructions to ensure efficient care.