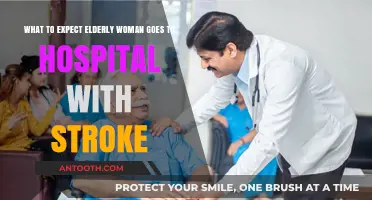
A hospital stay for esophageal varices, which are enlarged veins in the esophagus often caused by liver disease, typically involves close monitoring and specialized care to manage bleeding risks and underlying conditions. Patients can expect initial stabilization in an intensive care unit (ICU) or a dedicated gastrointestinal ward, where medical teams will administer medications like vasoconstrictors and antibiotics to control bleeding and prevent infection. Procedures such as endoscopic variceal ligation (EVL) or sclerotherapy may be performed to treat the varices directly. During the stay, patients will undergo frequent blood tests, imaging, and vital sign checks to assess liver function and overall health. Nutritionists may also provide dietary guidance to support recovery, and discussions about long-term management, including potential liver transplant evaluation, are common. The length of stay varies depending on the severity of the condition and response to treatment, with the primary goal being to stabilize the patient and prevent future complications.
| Characteristics | Values |
|---|---|
| Admission Reason | Bleeding esophageal varices (often due to portal hypertension from liver disease) |
| Length of Stay | Typically 2–7 days, depending on severity and complications |
| Initial Treatment | Endoscopic therapy (e.g., band ligation, sclerotherapy) to stop bleeding |
| Medications | Vasoconstrictors (e.g., octreotide), antibiotics, proton pump inhibitors |
| Monitoring | Frequent vital signs, hemoglobin/hematocrit levels, and fluid balance |
| Diet | Initially NPO (nothing by mouth), then advanced to soft or regular diet |
| IV Therapy | Intravenous fluids, blood transfusions if needed |
| Pain Management | Analgesics as needed for discomfort from procedures or complications |
| Complications | Re-bleeding, infection, aspiration pneumonia, fluid overload |
| Discharge Criteria | Stable vital signs, no active bleeding, tolerating oral diet |
| Follow-Up Care | Outpatient endoscopy, liver disease management, variceal surveillance |
| Patient Education | Signs of re-bleeding (e.g., vomiting blood, dark stools), medication adherence |
| Activity Restrictions | Avoid heavy lifting or straining for 1–2 weeks post-procedure |
| Emotional Support | Counseling or support groups for chronic liver disease patients |
| Prognosis | Depends on underlying liver function and response to treatment |
Explore related products





What You'll Learn
![]()
Admission process and initial assessment
Upon arrival at the hospital for esophageal varices, the admission process begins with a triage assessment to prioritize care based on the severity of symptoms. Patients presenting with acute variceal bleeding, a life-threatening condition, are immediately directed to the emergency department. Here, vital signs such as blood pressure, heart rate, and oxygen saturation are monitored to gauge hemodynamic stability. A brief medical history is taken, focusing on factors like liver disease, alcohol use, and prior episodes of bleeding. This initial evaluation is critical for determining the urgency of intervention and the need for intensive care unit (ICU) admission.
Following triage, a comprehensive initial assessment is conducted to identify the extent of the varices and the underlying cause. Diagnostic tools such as endoscopy are prioritized to visualize the esophageal varices and assess their size, location, and risk of rupture. Blood tests, including complete blood count (CBC), liver function tests, and coagulation profiles, are ordered to evaluate anemia, clotting abnormalities, and liver health. Imaging studies like abdominal ultrasounds may be performed to assess liver morphology and portal vein patency. This multifaceted approach ensures a precise understanding of the patient’s condition, guiding subsequent treatment decisions.
During this phase, patients are stabilized with immediate interventions to control bleeding and prevent complications. Intravenous fluids and blood transfusions are administered as needed to maintain hemodynamic stability. Vasoactive medications, such as octreotide (typically given as a 50 mcg bolus followed by a continuous infusion of 25–50 mcg/hour), are initiated to reduce portal pressure and decrease bleeding risk. Antibiotic prophylaxis, often with intravenous ceftriaxone (1–2 g daily), is started to prevent infection, a common complication in cirrhotic patients. These measures are tailored to the patient’s specific needs, balancing urgency with safety.
Practical tips for patients include arriving with a list of current medications, allergies, and recent procedures to expedite the admission process. Bringing a family member or caregiver can help ensure accurate communication of medical history. Patients should expect to remain nil per os (NPO) until the endoscopy is completed, as this is essential for safe sedation and procedural success. Clear, concise communication with the healthcare team about symptoms, such as vomiting blood or black stools, is vital for prompt and effective care. Understanding these steps can reduce anxiety and foster collaboration during a critical period.
Streamlining Hospital Efficiency: Strategies to Reduce Patient Waiting Times
You may want to see also
Explore related products





![]()
Diagnostic procedures (endoscopy, imaging) for varices evaluation
Endoscopy stands as the gold standard for diagnosing esophageal varices, offering a direct visualization of the esophageal lining and stomach. During this procedure, a thin, flexible tube equipped with a light and camera (endoscope) is gently inserted through the mouth and into the esophagus. This allows the gastroenterologist to assess the size, location, and severity of varices, which are crucial factors in determining treatment and risk of bleeding. For patients, the process typically takes 15–30 minutes, with mild sedation administered to ensure comfort. While the idea of an endoscope may sound intimidating, the procedure is minimally invasive and often well-tolerated, with most patients returning to normal activities within 24 hours.
Imaging studies, such as abdominal ultrasound or CT scans, play a complementary role in varices evaluation, particularly in assessing the underlying cause of portal hypertension. Ultrasound, for instance, can visualize the liver, spleen, and portal vein, providing insights into liver health and blood flow dynamics. CT scans offer a more detailed view of the abdominal anatomy, helping identify complications like ascites or liver cirrhosis. These imaging modalities are non-invasive and typically painless, though CT scans may involve exposure to radiation and the use of contrast dye, which requires careful consideration in patients with kidney issues. While imaging alone cannot diagnose varices, it provides essential context for understanding the broader clinical picture.
A key advantage of endoscopy over imaging is its ability to perform therapeutic interventions during the same session. For instance, if large, high-risk varices are detected, the endoscopist can immediately apply band ligation—a procedure where small rubber bands are placed around the varices to cut off blood supply and prevent rupture. This dual diagnostic-therapeutic capability makes endoscopy not just a diagnostic tool but a potentially life-saving intervention. Patients scheduled for endoscopy should follow pre-procedure instructions carefully, such as fasting for 6–8 hours beforehand, to ensure optimal visualization and safety.
Comparatively, while imaging provides valuable systemic information, it lacks the precision and immediacy of endoscopy for varices evaluation. For example, an ultrasound might suggest portal hypertension, but only endoscopy can confirm the presence and severity of varices. This distinction underscores the importance of a tailored diagnostic approach, where imaging supports but does not replace endoscopic evaluation. Patients with suspected varices should expect a multidisciplinary assessment, combining endoscopy for direct visualization and imaging for contextual understanding, to guide effective management and prevention strategies.
Hospitals in the US: A Comprehensive Count
You may want to see also
Explore related products

$17.97





![]()
Treatment options (banding, medication, TIPS) during stay
Esophageal varices, swollen veins in the esophagus often due to liver disease, require prompt treatment to prevent life-threatening bleeding. During a hospital stay, patients can expect a tailored approach to manage these varices, with treatment options including endoscopic banding, medication, and transjugular intrahepatic portosystemic shunt (TIPS). Each method addresses the condition differently, and the choice depends on the severity of the varices, the patient’s overall health, and the risk of complications.
Endoscopic Banding: A Frontline Intervention
For patients with medium to large varices or those who have already experienced bleeding, endoscopic banding is often the first-line treatment. This minimally invasive procedure involves placing small rubber bands around the varices to cut off their blood supply, causing them to shrink and eventually scar. Typically performed under sedation, the procedure takes 15–30 minutes, and patients can expect to remain in the hospital for observation afterward. Multiple sessions, spaced 1–2 weeks apart, are usually required to fully eradicate the varices. While effective, banding carries a small risk of bleeding (2–5%) or infection, so close monitoring is essential.
Medication Management: A Complementary Strategy
Medications play a crucial role in reducing portal hypertension, the underlying cause of esophageal varices. Nonselective beta-blockers, such as propranolol or nadolol, are commonly prescribed to lower blood pressure in the portal vein. Dosages are individualized, often starting at 20–40 mg daily for propranolol and titrated up to 160 mg or higher based on tolerance and heart rate response. For patients who cannot tolerate beta-blockers, nitrates like isosorbide mononitrate (20–60 mg daily) may be used, though they are less effective. These medications are typically initiated during the hospital stay and continued long-term to prevent rebleeding. Adherence is critical, as discontinuation can lead to rebound hypertension and increased bleeding risk.
TIPS: A Salvage Option for High-Risk Cases
When banding and medication fail to control bleeding, or in patients with recurrent variceal hemorrhage, TIPS may be considered. This interventional radiology procedure creates a shunt between the portal and hepatic veins, reducing pressure in the portal system. While highly effective in stopping acute bleeding (success rates >90%), TIPS carries significant risks, including hepatic encephalopathy (30–50% of cases) and liver failure, particularly in patients with advanced liver disease. The procedure is performed under local anesthesia with mild sedation and requires a hospital stay of 1–2 days for monitoring. TIPS is often reserved for younger patients (under 70) with better liver function, as older patients or those with severe cirrhosis may not tolerate the procedure well.
Practical Tips for Patients
During a hospital stay, patients should expect frequent monitoring of vital signs, blood tests to assess liver function, and dietary adjustments to manage symptoms. Clear communication with the healthcare team is essential, as treatment decisions are often made collaboratively. Patients undergoing banding should avoid aspirin or NSAIDs for at least 48 hours post-procedure to minimize bleeding risk. For those on beta-blockers, monitoring for side effects like fatigue, dizziness, or shortness of breath is crucial. After TIPS, patients will need regular follow-up imaging to ensure shunt patency and manage complications. Understanding these treatment options empowers patients to actively participate in their care and improve outcomes.
Key Factors Leading to Hospital Readmissions from Skilled Nursing Facilities
You may want to see also
Explore related products






![]()
Monitoring and managing complications (bleeding, infection)
Active monitoring for bleeding and infection is a cornerstone of managing esophageal varices during a hospital stay. Continuous vital sign monitoring, including blood pressure, heart rate, and hemoglobin levels, is essential to detect early signs of bleeding. Patients are often placed on telemetry to track cardiac stability, as hypovolemia from bleeding can lead to tachycardia or hypotension. Blood tests, such as complete blood counts and coagulation profiles, are repeated at regular intervals to assess for ongoing blood loss or clotting abnormalities. For high-risk patients, endoscopic surveillance may be scheduled to visually inspect the varices and intervene if necessary.
Infection prevention is equally critical, as hospitalized patients with esophageal varices are often immunocompromised due to underlying liver disease. Strict aseptic techniques are employed during procedures, and patients may receive prophylactic antibiotics, such as intravenous ceftriaxone (1g daily), to reduce the risk of spontaneous bacterial peritonitis or other infections. Hand hygiene protocols are rigorously enforced for all healthcare personnel, and patients are educated on recognizing early signs of infection, such as fever, chills, or abdominal pain. Wound care, if applicable, is meticulous, with daily dressing changes and monitoring for erythema or discharge.
Bleeding complications require swift intervention, often starting with resuscitation to stabilize hemodynamics. Intravenous fluids, blood transfusions, and vasopressors like terlipressin (1–2 mg every 4–6 hours) may be administered to maintain perfusion. Endoscopic therapy, such as band ligation or sclerotherapy, is typically performed within 12–24 hours to control active bleeding. In severe cases, transjugular intrahepatic portosystemic shunt (TIPS) may be considered to reduce portal pressure. Patients are closely observed post-procedure for rebleeding, with repeat endoscopy scheduled if necessary.
Managing infection involves prompt identification and targeted treatment. Empirical broad-spectrum antibiotics, such as piperacillin-tazobactam (4.5 g every 6 hours), are initiated if infection is suspected, with de-escalation based on culture results. Diagnostic paracentesis is performed in patients with ascites to rule out spontaneous bacterial peritonitis, which requires specific antibiotic coverage. Fever workups, including blood cultures and chest X-rays, are standard to identify the source of infection. Patients with recurrent infections may require long-term prophylactic antibiotics or referral to infectious disease specialists.
Practical tips for patients include adhering to a low-sodium diet to minimize ascites, avoiding nonsteroidal anti-inflammatory drugs (NSAIDs) that can worsen bleeding risk, and reporting any symptoms like black stools, abdominal pain, or fever immediately. Caregivers should be trained to monitor for subtle signs of complications, such as confusion (hepatic encephalopathy) or jaundice (worsening liver function). Discharge planning includes arranging follow-up appointments, ensuring access to medications, and providing clear instructions on when to seek emergency care. Proactive management of bleeding and infection not only improves outcomes but also reduces the likelihood of readmission.
Enrolling in VA Hospital: A Simple Guide
You may want to see also
Explore related products






![]()
Discharge planning and follow-up care instructions
Before leaving the hospital after treatment for esophageal varices, patients receive a detailed discharge plan to ensure a smooth transition to home care. This plan typically includes medication schedules, dietary guidelines, and activity restrictions. For instance, beta-blockers like propranolol may be prescribed to reduce portal pressure, often starting at 20–40 mg twice daily, with dosage adjustments based on heart rate and blood pressure. Patients must adhere strictly to these instructions to prevent rebleeding, a common complication with a recurrence rate of up to 60% within two years.
Dietary modifications play a critical role in post-discharge care. Patients are advised to adopt a low-sodium diet, limiting intake to 2,000 mg per day, to minimize fluid retention and reduce pressure on the varices. Small, frequent meals are recommended to avoid distending the stomach, which can increase esophageal pressure. Avoiding alcohol is non-negotiable, as it exacerbates liver damage and increases the risk of variceal bleeding. A registered dietitian often provides personalized meal plans to ensure nutritional needs are met while adhering to these restrictions.
Follow-up care is essential to monitor healing and prevent complications. Patients typically have an endoscopy scheduled 6–8 weeks post-discharge to assess variceal status and determine the need for further interventions, such as band ligation. Regular liver function tests and imaging studies, like ultrasounds, may also be ordered to evaluate liver health and portal hypertension. Missing these appointments can delay detection of recurrent varices or other issues, increasing the risk of severe bleeding or liver failure.
Practical tips for home care include keeping a symptom journal to track changes in appetite, energy levels, or signs of bleeding (e.g., dark stools or vomiting blood). Patients should also have a clear understanding of when to seek emergency care, such as sudden dizziness, confusion, or severe abdominal pain. Caregivers or family members should be educated on these warning signs and the importance of medication adherence. Finally, emotional support is crucial, as the chronic nature of esophageal varices can lead to anxiety or depression, which may impact recovery.
Bozeman Deaconess Hospital: Private or Public?
You may want to see also
Frequently asked questions
Esophageal varices are enlarged veins in the esophagus, often caused by liver disease or portal hypertension. A hospital stay may be necessary if they rupture and cause bleeding, requiring emergency treatment to stop the bleeding and stabilize the patient.
Treatments may include endoscopic procedures like band ligation to stop bleeding, medications to reduce portal pressure (e.g., beta-blockers), and, in severe cases, a transjugular intrahepatic portosystemic shunt (TIPS) to redirect blood flow.
The length of stay varies depending on the severity of bleeding and response to treatment. It can range from a few days to over a week, especially if complications arise or additional procedures are needed.
You will be closely monitored for signs of ongoing bleeding, such as blood in vomit or stool, low blood pressure, and decreased hemoglobin levels. Vital signs, lab tests, and imaging may also be performed regularly.
After discharge, you’ll likely need follow-up appointments to monitor your condition, adjust medications, and discuss long-term management strategies, such as lifestyle changes or further interventions to prevent future bleeding.


![The Ultimate Hospital Stay Activity Book For Adults: XXL Large Print Relaxing Activities, Memory Games & Brain Puzzles for Patients and Families [1-2 Players!]](https://m.media-amazon.com/images/I/61aUayZHnXL._AC_UY218_.jpg)