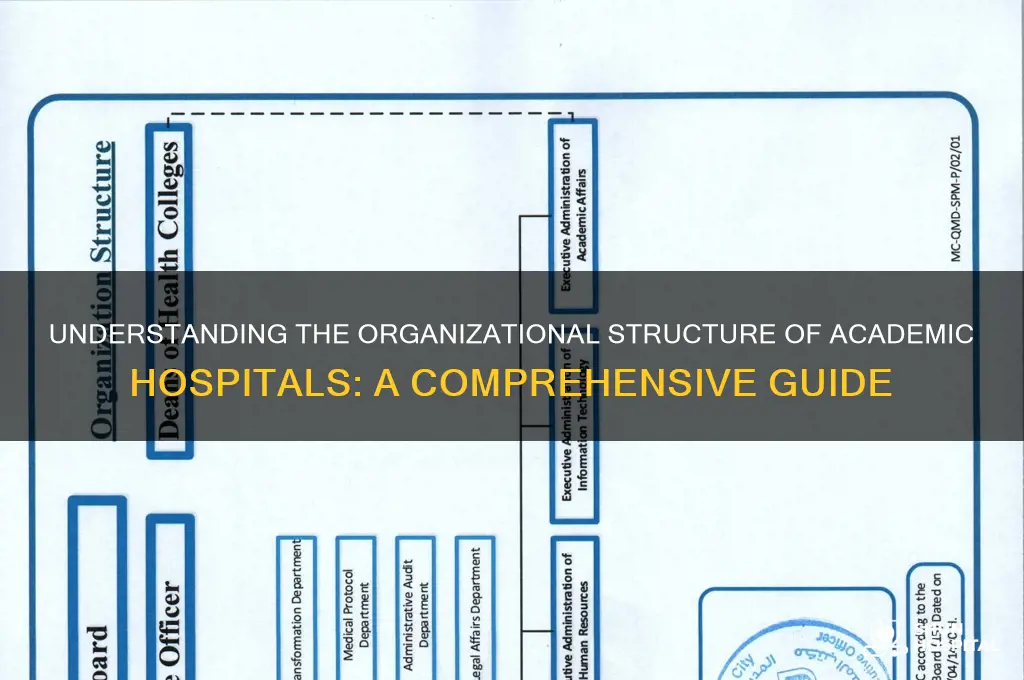
An academic hospital operates under a complex organizational structure that blends clinical care, education, and research, typically characterized by a matrix or hybrid model. At its core, it is often structured hierarchically, with top-level leadership including a CEO, Chief Medical Officer, and Deans overseeing operations, medical services, and academic programs, respectively. Departments such as surgery, internal medicine, and pediatrics function semi-autonomously, led by chairs or chiefs who manage clinical activities while collaborating with academic faculty to integrate teaching and research. Additionally, interdisciplinary committees and councils ensure alignment between clinical, educational, and research objectives, fostering a culture of innovation and evidence-based practice. This structure enables academic hospitals to fulfill their tripartite mission of delivering high-quality patient care, training future healthcare professionals, and advancing medical knowledge through cutting-edge research.
Explore related products



$49.62 $63



What You'll Learn
- Hierarchical Structure: Clear chain of command, with departments like administration, clinical, and research
- Functional Departments: Specialized units (e.g., surgery, pediatrics) operate independently under central leadership
- Matrix Structure: Dual reporting lines, combining clinical roles with administrative or research responsibilities
- Decentralized Model: Autonomous departments manage operations, with minimal central oversight for flexibility
- Hybrid Structure: Combines hierarchical and decentralized elements to balance control and departmental autonomy
![]()
Hierarchical Structure: Clear chain of command, with departments like administration, clinical, and research
Academic hospitals, as complex entities, often adopt a hierarchical structure to manage their multifaceted operations. This model establishes a clear chain of command, ensuring accountability and efficiency across diverse departments. At the apex typically resides a board of directors or senior leadership team, comprising individuals with expertise in healthcare administration, finance, and strategic planning. They set the overall vision, allocate resources, and oversee the hospital's performance.
Beneath this executive level, the hierarchy branches into distinct departments, each with its own leadership and specialized functions. Administration forms the backbone, handling finance, human resources, legal matters, and facility management. This department ensures the hospital operates within budgetary constraints, complies with regulations, and maintains a functional infrastructure.
Clinical departments, the heart of patient care, are further subdivided into specialties like internal medicine, surgery, pediatrics, and obstetrics/gynecology. Each department is led by a department chair, often a senior physician, who oversees clinical operations, research activities within their specialty, and the professional development of staff.
Research, a cornerstone of academic hospitals, operates as a distinct department, fostering innovation and advancing medical knowledge. This department is typically headed by a research director, responsible for securing funding, managing research projects, and ensuring ethical conduct.
This hierarchical structure offers several advantages. Firstly, it promotes clear lines of authority and responsibility, minimizing confusion and streamlining decision-making. Secondly, it facilitates specialization, allowing departments to focus on their core competencies, be it patient care, administration, or research. This specialization fosters expertise and efficiency within each domain.
However, a rigid hierarchy can also present challenges. Communication across departments can become siloed, hindering collaboration and potentially leading to inefficiencies. Additionally, the top-down decision-making process may limit input from frontline staff, potentially overlooking valuable insights.
To mitigate these challenges, successful academic hospitals foster a culture of open communication and interdisciplinary collaboration. Regular meetings, cross-departmental committees, and shared decision-making platforms encourage information flow and ensure that diverse perspectives are considered. Furthermore, empowering employees at all levels through training and development opportunities can enhance their ability to contribute meaningfully to the organization's success.
In essence, while the hierarchical structure provides a necessary framework for managing the complexity of academic hospitals, its effectiveness hinges on fostering a culture of collaboration and communication that transcends departmental boundaries.
Hospital ER Visiting Hours: When Do They End?
You may want to see also
Explore related products

$54.03 $89




![]()
Functional Departments: Specialized units (e.g., surgery, pediatrics) operate independently under central leadership
Academic hospitals often adopt a functional organizational structure, where specialized departments like surgery, pediatrics, or cardiology operate as semi-autonomous units under a central administrative leadership. This model leverages the expertise of each department while maintaining overarching governance to ensure alignment with institutional goals. For instance, a pediatric department might independently manage its patient care protocols, research initiatives, and staff training, but it adheres to hospital-wide policies on budgeting, compliance, and strategic planning. This balance allows for both specialization and cohesion, critical in complex healthcare environments.
Consider the operational dynamics of this structure. Each functional department typically has its own leadership—a department chair or director—who oversees day-to--day activities, resource allocation, and performance metrics. These leaders report to a central authority, such as a hospital CEO or board, which sets broad directives and ensures consistency across departments. For example, while the surgery department may decide on specific surgical techniques or equipment purchases, it must align with the hospital’s financial constraints and quality standards. This layered accountability fosters efficiency without sacrificing institutional unity.
One of the key advantages of this structure is its ability to support specialized innovation. Departments can focus on their core competencies, driving advancements in patient care, research, and education. For instance, a pediatrics department might pioneer new treatment protocols for childhood asthma, while the surgery department develops minimally invasive techniques. However, this specialization requires careful coordination to avoid silos. Regular interdepartmental collaboration—through joint committees or shared projects—is essential to ensure that innovations benefit the hospital as a whole, not just individual units.
Despite its benefits, the functional structure is not without challenges. Resource allocation often becomes a point of contention, as departments compete for funding, staff, and facilities. Central leadership must employ transparent criteria to distribute resources fairly, balancing the needs of high-revenue departments like surgery with those of less profitable but critical areas like psychiatry. Additionally, maintaining consistent patient care standards across departments can be difficult, requiring robust oversight mechanisms such as quality improvement teams or standardized protocols.
In practice, academic hospitals can optimize this structure by fostering a culture of shared purpose. While departments operate independently, they must recognize their role in the larger mission of the hospital—whether it’s advancing medical knowledge, training future healthcare leaders, or providing community care. For example, a hospital might implement cross-departmental training programs or encourage collaborative research projects to strengthen interdepartmental ties. By aligning autonomy with collective goals, the functional structure can maximize both specialization and unity, making it a powerful model for academic healthcare institutions.
Albany Medical Center: A Comprehensive Healthcare Facility
You may want to see also
Explore related products






![]()
Matrix Structure: Dual reporting lines, combining clinical roles with administrative or research responsibilities
Academic hospitals often adopt a matrix structure to balance clinical, administrative, and research demands. This model creates dual reporting lines, allowing professionals to combine their clinical roles with administrative or research responsibilities. For instance, a cardiologist might report to both the head of cardiology and the director of clinical research, ensuring their expertise contributes to patient care and scientific advancement simultaneously. This duality fosters collaboration but requires clear communication to avoid role ambiguity.
Implementing a matrix structure involves strategic role design. Start by identifying key personnel whose skills span clinical and non-clinical domains, such as a surgeon with a background in health policy. Assign them to cross-functional teams, like a committee developing evidence-based treatment protocols. Use tools like RACI matrices (Responsible, Accountable, Consulted, Informed) to clarify responsibilities and prevent overlap. For example, a physician leading a research trial should be "Accountable" for its outcomes but only "Consulted" on budget approvals, which fall under the finance department’s purview.
One challenge of this structure is managing competing priorities. A physician juggling patient rounds, grant proposals, and departmental meetings may face burnout. To mitigate this, establish boundaries such as protected research time (e.g., 20% of work hours dedicated to non-clinical tasks) or administrative support for scheduling. For instance, Mayo Clinic’s matrix model includes research coordinators who handle paperwork, freeing clinicians to focus on high-impact activities. Regular check-ins with both reporting managers can also help align expectations and redistribute workloads as needed.
The benefits of a matrix structure are evident in institutions like Johns Hopkins Hospital, where clinicians contribute to groundbreaking research while maintaining patient care standards. This model accelerates translational research, as insights from the bedside directly inform studies. For example, a neurologist involved in both clinical practice and drug trials can identify patient needs more effectively, leading to targeted research questions. However, success hinges on fostering a culture of mutual respect between clinical and non-clinical leaders, ensuring neither role overshadows the other.
To sustain a matrix structure, continuous evaluation is critical. Track metrics such as publication rates, patient outcomes, and employee satisfaction to gauge effectiveness. For instance, if research productivity drops, reassess time allocations or provide additional training. Conversely, if clinical quality suffers, rebalance responsibilities. Case studies from institutions like Massachusetts General Hospital show that periodic restructuring—such as rotating leadership roles every 2–3 years—keeps the system dynamic and responsive to evolving needs. By embracing flexibility, academic hospitals can maximize the strengths of a matrix model while minimizing its complexities.
Hospital Bag Essentials: What Guys Should Pack for the Birth
You may want to see also
Explore related products






![]()
Decentralized Model: Autonomous departments manage operations, with minimal central oversight for flexibility
Academic hospitals often grapple with balancing specialized care, research, and education, making their organizational structure critical. One approach gaining traction is the decentralized model, where departments operate autonomously with minimal central oversight. This structure empowers departments like cardiology, oncology, or pediatrics to make decisions tailored to their unique needs, fostering innovation and responsiveness. For instance, a cardiology department might allocate more resources to cutting-edge research, while pediatrics focuses on patient-centered care initiatives. This flexibility allows departments to adapt quickly to evolving medical landscapes, such as implementing new treatment protocols or expanding telehealth services without waiting for central approval.
However, decentralization isn’t without challenges. Without robust coordination mechanisms, departments may duplicate efforts or operate in silos, hindering collaboration. For example, two departments might independently purchase similar medical equipment, leading to inefficiencies. To mitigate this, academic hospitals adopting this model often establish cross-departmental committees or shared governance structures. These ensure alignment on strategic goals while preserving departmental autonomy. Additionally, clear communication channels and shared digital platforms can facilitate resource sharing and knowledge exchange, reducing redundancy.
A key advantage of the decentralized model is its ability to enhance departmental accountability. When departments manage their budgets, staffing, and operations, they are more likely to take ownership of outcomes. For instance, a radiology department might streamline its workflow to reduce wait times, directly impacting patient satisfaction. This accountability extends to research and education, where departments can allocate resources to initiatives that align with their strengths and priorities. However, central leadership must still provide oversight to ensure compliance with regulatory standards and institutional values, striking a balance between freedom and accountability.
Implementing a decentralized model requires careful planning and cultural shifts. Leadership must foster a mindset of trust and collaboration, encouraging departments to view autonomy as a tool for collective success rather than isolation. Training programs can help department heads develop leadership and financial management skills, ensuring they are equipped to handle increased responsibilities. For example, a workshop on budget management tailored for clinical leaders can empower them to make informed financial decisions. Over time, this model can transform academic hospitals into agile, innovative hubs where departments thrive independently while contributing to the institution’s overarching mission.
Ultimately, the decentralized model offers academic hospitals a pathway to flexibility and innovation, but its success hinges on thoughtful implementation and ongoing refinement. By empowering departments to manage their operations while maintaining strategic alignment, hospitals can navigate the complexities of modern healthcare more effectively. This approach not only enhances departmental performance but also positions the institution to adapt to future challenges, ensuring it remains a leader in patient care, research, and education.
The Impact of COVID-19 Hospitalizations Globally
You may want to see also
Explore related products




![Hierarchy of Evil [DVD]](https://m.media-amazon.com/images/I/615GKX55ReL._AC_UY218_.jpg)

![]()
Hybrid Structure: Combines hierarchical and decentralized elements to balance control and departmental autonomy
Academic hospitals often grapple with the tension between centralized control and departmental autonomy. A hybrid structure emerges as a pragmatic solution, blending hierarchical oversight with decentralized decision-making to navigate this complexity. At its core, this model acknowledges the dual nature of academic healthcare: the need for standardized protocols and the value of specialized expertise. For instance, while administrative functions like budgeting and compliance remain centralized, clinical departments retain autonomy in patient care and research initiatives. This balance ensures that the hospital operates efficiently while fostering innovation and adaptability.
Consider the implementation of a hybrid structure in a large academic medical center. The executive leadership sets overarching strategic goals, such as reducing readmission rates by 15% within two years. However, individual departments like cardiology or oncology are empowered to design tailored interventions—whether through telemedicine follow-ups or multidisciplinary care teams. This approach leverages the hospital’s scale while allowing departments to address unique patient populations and clinical challenges. Key to success is clear communication: quarterly meetings between leadership and department heads ensure alignment without stifling creativity.
One cautionary note: hybrid structures require robust governance mechanisms to prevent silos or conflicting priorities. For example, a neurology department might prioritize cutting-edge research, while the finance team focuses on cost containment. To mitigate this, establish cross-functional committees that include representatives from clinical, administrative, and research domains. These committees can adjudicate resource allocation, ensuring that departmental autonomy doesn’t undermine institutional goals. Additionally, performance metrics should be both institution-wide (e.g., patient satisfaction scores) and department-specific (e.g., publication output for research units).
A persuasive argument for the hybrid model lies in its ability to attract and retain top talent. Clinician-scientists, for instance, are more likely to thrive in an environment where they have autonomy over their research agendas while benefiting from institutional support for grant applications and regulatory compliance. Similarly, nurses and allied health professionals appreciate decentralized decision-making that allows them to tailor care protocols to their patient populations. By offering this flexibility, academic hospitals position themselves as employers of choice in a competitive healthcare landscape.
In practice, transitioning to a hybrid structure involves deliberate steps. Start by mapping current workflows to identify areas where decentralization can improve efficiency—for example, allowing departments to manage their own supply chains for specialized equipment. Next, invest in training for middle managers, who play a critical role in bridging centralized policies and departmental execution. Finally, pilot the model in one or two departments before scaling institution-wide. This phased approach minimizes disruption and allows for course correction based on real-world feedback.
The takeaway is clear: a hybrid structure isn’t a one-size-fits-all solution but a dynamic framework tailored to the unique demands of academic hospitals. By combining hierarchical control with departmental autonomy, it fosters a culture of accountability and innovation. Hospitals that adopt this model position themselves to deliver high-quality care, advance medical knowledge, and adapt to the evolving healthcare landscape—all while maintaining the operational rigor required of complex institutions.
Exploring Diverse Careers in Hospitality and Tourism: Opportunities and Roles
You may want to see also
Frequently asked questions
Academic hospitals often operate under a matrix organizational structure, combining functional and divisional structures. This allows for collaboration between clinical departments, research units, and educational programs while maintaining specialized expertise.
Unlike non-academic hospitals, which may focus solely on patient care, academic hospitals integrate clinical care, research, and education. Their structure often includes additional layers for research departments, teaching programs, and affiliations with medical schools.
The Chief Executive Officer (CEO) or Hospital Director usually holds the highest authority, overseeing operations, finances, and strategic planning. However, academic hospitals also have strong influence from Deans of Medical Schools and Department Chairs due to their educational and research mandates.
Departments are typically organized by medical specialties (e.g., cardiology, neurology) and functional areas (e.g., research, education). Each department may have its own leadership, such as a Department Chair, who reports to higher administrative levels while collaborating across disciplines.







![Woman hierarchy bottom girl [DVD] Hieralkey JAPANESE EDITION](https://m.media-amazon.com/images/I/51fzxtE03gL._AC_UY218_.jpg)



















