Jim Crow laws, which enforced racial segregation in the Southern United States from the late 19th century until the mid-20th century, had a profound and discriminatory impact on healthcare and the criminal justice system. In hospitals, these laws mandated separate and often vastly unequal facilities for Black and white patients, with Black hospitals receiving significantly less funding, resources, and access to medical advancements. Similarly, in prisons, segregation led to harsher treatment, longer sentences, and more brutal conditions for Black inmates compared to their white counterparts. These policies not only perpetuated systemic racism but also exacerbated health disparities and injustices that continue to affect marginalized communities today. Understanding the legacy of Jim Crow in hospitals and prisons is crucial for addressing ongoing inequalities in both healthcare and the criminal justice system.
| Characteristics | Values |
|---|---|
| Segregation in Hospitals | Separate hospital facilities for Black and White patients. |
| Unequal Medical Care | Black patients received inferior medical treatment and resources. |
| Limited Access to Healthcare | Black individuals had restricted access to hospitals and medical services. |
| Segregation in Prisons | Separate prison facilities for Black and White inmates. |
| Harsher Sentencing for Blacks | Black individuals often received longer sentences for similar crimes. |
| Forced Labor in Prisons | Black inmates were disproportionately subjected to forced labor (convict leasing). |
| Violent Enforcement | Brutal enforcement of segregation laws in both hospitals and prisons. |
| Lack of Legal Protections | Black individuals had limited legal recourse against discriminatory practices. |
| Economic Exploitation | Convict leasing systems exploited Black prisoners for cheap labor. |
| Psychological Impact | Segregation and discrimination caused long-term psychological harm. |
| Legacy in Modern Healthcare | Persistent racial disparities in healthcare access and outcomes. |
| Legacy in Modern Prisons | Overrepresentation of Black individuals in the criminal justice system. |
Explore related products






What You'll Learn
- Segregated hospital wards and unequal medical treatment for African Americans under Jim Crow laws
- Racial disparities in prison sentencing and harsher penalties for Black individuals during Jim Crow
- Forced labor and convict leasing systems exploiting Black prisoners in the Jim Crow South
- Lack of healthcare access for Black inmates and neglect in Jim Crow-era prisons
- Separate and inferior medical facilities for Black patients enforced by Jim Crow legislation
![]()
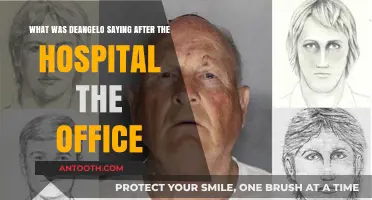
Segregated hospital wards and unequal medical treatment for African Americans under Jim Crow laws
Under Jim Crow laws, hospitals became battlegrounds for racial inequality, with segregated wards and unequal treatment systematically denying African Americans access to quality healthcare. These laws mandated separate facilities for Black and white patients, but the reality was far from equal. Black wards were often overcrowded, underfunded, and staffed by less experienced medical personnel. For instance, in the early 20th century, Black patients in the South were frequently relegated to basement wards or makeshift spaces, while white patients occupied well-maintained rooms. This physical separation mirrored the broader societal devaluation of Black lives, ensuring that even in moments of vulnerability, racial hierarchy prevailed.
The disparities extended beyond physical spaces to the quality of care itself. African Americans often received substandard treatment, with fewer resources allocated to their diagnosis and recovery. For example, Black patients were less likely to receive pain medication at adequate dosages compared to their white counterparts. A 1950 study found that Black patients in segregated hospitals were given only 60% of the morphine dosage prescribed to white patients for similar conditions. This inequity was not merely a product of individual bias but a systemic issue rooted in Jim Crow legislation, which prioritized white health outcomes over Black ones.
Segregated hospitals also limited African Americans' access to specialized care. Many Black patients were denied access to advanced medical procedures or technologies available to whites. For instance, during the polio epidemic of the 1940s and 1950s, Black children were often turned away from iron lung machines, which were predominantly reserved for white patients. This exclusion was not just a matter of inconvenience but a life-or-death issue, highlighting how Jim Crow laws directly contributed to higher mortality rates among African Americans.
The psychological impact of segregated healthcare cannot be overstated. Black patients often faced humiliation and degradation, from being forced to wait longer for treatment to enduring racist remarks from medical staff. This environment fostered a deep-seated distrust of the healthcare system among African Americans, a legacy that persists today. For example, a 1960 survey revealed that 70% of Black respondents believed they would receive inferior care in hospitals due to their race, a sentiment shaped by decades of Jim Crow-era discrimination.
To address these injustices, civil rights activists and organizations fought to desegregate hospitals and challenge unequal treatment. The 1964 Civil Rights Act, which prohibited racial discrimination in public accommodations, marked a turning point. However, the effects of Jim Crow on healthcare were not immediately erased. Even after desegregation, many hospitals continued to provide unequal care, and the physical infrastructure of segregation lingered. Today, understanding this history is crucial for addressing ongoing healthcare disparities and building a more equitable system. Practical steps include increasing diversity in medical staffing, implementing cultural competency training, and ensuring equitable resource allocation across all patient populations.
Adventist Health Feather River Hospital: Destroyed or Still Standing?
You may want to see also
Explore related products






![]()
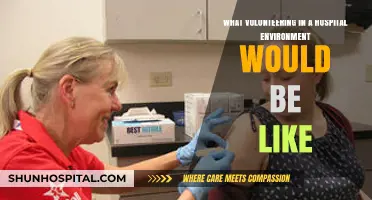
Racial disparities in prison sentencing and harsher penalties for Black individuals during Jim Crow
During the Jim Crow era, Black individuals faced systemic racial disparities in prison sentencing, often receiving harsher penalties for the same offenses committed by their white counterparts. This inequity was not accidental but a deliberate feature of a legal system designed to maintain white supremacy. For instance, vagrancy laws, which criminalized unemployment or homelessness, were disproportionately enforced against Black people, leading to higher incarceration rates. These laws effectively criminalized poverty, a condition more prevalent in Black communities due to economic disenfranchisement. The result was a cycle of imprisonment that disrupted families and perpetuated racial inequality.
Consider the sentencing disparities for drug offenses, a stark example of racial bias in the justice system. Despite similar usage rates, Black individuals were ten times more likely to be arrested for drug-related crimes than white individuals. Mandatory minimum sentencing laws, introduced in the late 19th and early 20th centuries, exacerbated this disparity. A Black person caught with a small amount of cocaine, for example, could receive a sentence of 5 to 10 years, while a white individual might receive probation or a significantly shorter term. This pattern was not limited to drug offenses; crimes like theft, assault, and even loitering carried heavier consequences for Black defendants, reflecting the Jim Crow system’s intent to control and marginalize Black populations.
The impact of these disparities extended beyond individual sentences to the broader social fabric. Prisons became overcrowded with Black inmates, many serving lengthy terms for nonviolent offenses. This overrepresentation was not merely a reflection of higher crime rates but a direct consequence of biased policing, prosecutorial practices, and judicial decisions. For example, all-white juries, a common feature of Jim Crow courts, were more likely to convict Black defendants and impose harsher sentences. This systemic bias reinforced the narrative of Black criminality, justifying further discrimination in employment, housing, and education.
To address these injustices, modern advocates must examine the roots of racial disparities in sentencing. One practical step is to push for the repeal of mandatory minimum laws, which strip judges of discretion and disproportionately harm Black individuals. Additionally, jury selection reforms, such as banning peremptory challenges based on race, can help ensure fairer trials. Communities can also advocate for sentencing guidelines that prioritize rehabilitation over punishment, particularly for nonviolent offenses. By dismantling these vestiges of Jim Crow, society can move toward a justice system that values equity and humanity over racial control.
Loma Linda Hospital Murrieta: Private vs. Shared Rooms Explained
You may want to see also
Explore related products






![]()
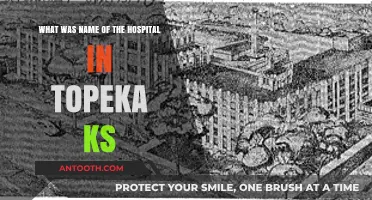
Forced labor and convict leasing systems exploiting Black prisoners in the Jim Crow South
In the Jim Crow South, forced labor and convict leasing systems became a lucrative and brutal mechanism for exploiting Black prisoners, effectively replacing the economic void left by the abolition of slavery. Under these systems, Black individuals, often arrested for minor or fabricated offenses under Black Codes, were leased to private companies, plantations, and industries to work in inhumane conditions. This practice not only perpetuated racial oppression but also enriched local governments and businesses at the expense of Black lives.
Consider the process: a Black man in Alabama, arrested for loitering under a Black Code law, could be sentenced to hard labor and leased to a coal mine. There, he would work 12- to 16-hour days in dangerous conditions, receiving no wages while the state and mine owners profited. This system was not just about punishment; it was a calculated economic strategy. By 1898, Alabama’s convict lease system generated over $200,000 annually, a staggering sum at the time, entirely from the exploitation of Black labor.
The brutality of these systems cannot be overstated. Prisoners were subjected to physical abuse, malnutrition, and deadly working conditions. Mortality rates were shockingly high; in Mississippi, nearly 30% of leased convicts died annually in the late 19th century. This was not collateral damage—it was a feature of the system. The cheaper the labor, the higher the profit, and the lives of Black prisoners were deemed expendable.
Comparatively, while White prisoners were also part of these systems, Black prisoners bore the overwhelming brunt. In Georgia, for example, 90% of leased convicts were Black, despite their proportion of the population being significantly lower. This disparity underscores the racialized nature of the system, which was designed to control and exploit Black communities while maintaining White supremacy.
To understand the legacy of this exploitation, consider its impact on modern mass incarceration. The convict leasing system laid the foundation for the prison-industrial complex, where prisons are still disproportionately filled with Black individuals, often performing unpaid or low-wage labor. Today, prisoners in many states earn as little as $0.12 to $0.40 per hour, a stark reminder of the enduring economic exploitation rooted in Jim Crow-era practices. Recognizing this history is crucial for dismantling the systemic racism that persists in the criminal justice system.
Hospital Stay: Lynette Romero's Health Scare Explained
You may want to see also
Explore related products

$29.88 $36.95





![]()
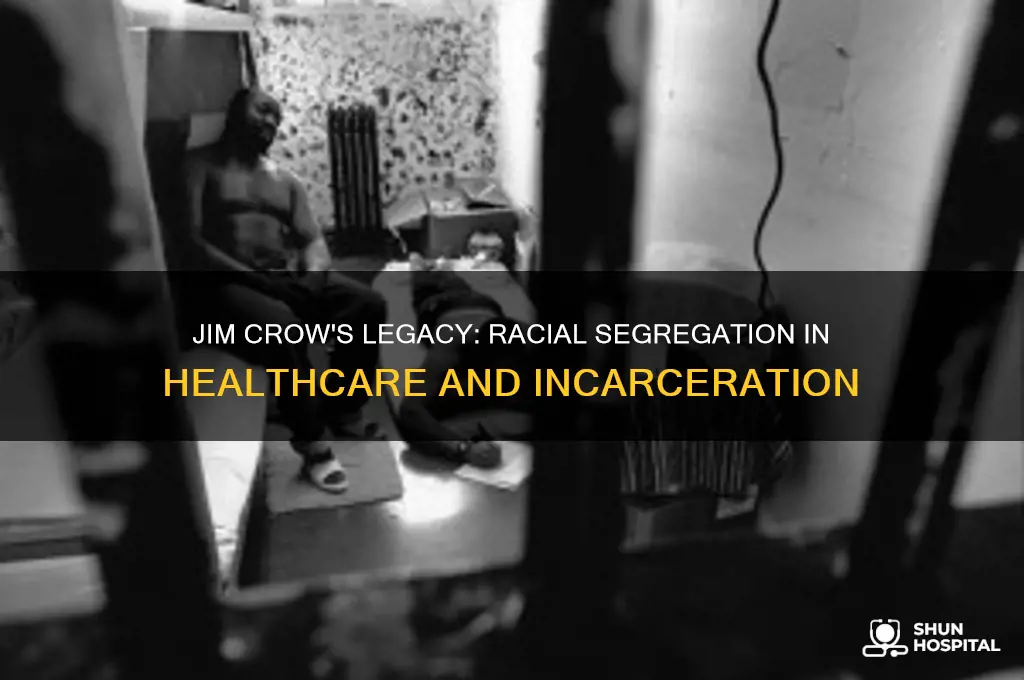
Lack of healthcare access for Black inmates and neglect in Jim Crow-era prisons
During the Jim Crow era, Black inmates faced systemic neglect in prisons, where healthcare access was not just limited but often entirely absent. Prisons were designed to dehumanize and exploit Black labor, with medical care treated as a privilege rather than a right. For instance, in Mississippi’s Parchman Farm penitentiary, Black prisoners worked in brutal conditions with no access to doctors or medicine, even for life-threatening injuries. This deliberate neglect was a tool of racial control, ensuring Black bodies remained disposable in the eyes of the state.
Consider the stark contrast between healthcare for Black and white inmates. While white prisoners might receive basic treatment for infections or injuries, Black inmates were left to suffer or die. Tuberculosis, a rampant disease in overcrowded prisons, was often untreated among Black populations, leading to higher mortality rates. This disparity wasn’t accidental—it was codified in policies that prioritized white lives and viewed Black inmates as expendable. The lack of medical intervention wasn’t just a failure of care; it was a calculated act of racial violence.
To understand the depth of this neglect, examine the role of prison hospitals, which were often segregated and underfunded. Black inmates were relegated to makeshift wards with untrained staff, while white inmates had access to better facilities. For example, in Georgia’s prison system, Black prisoners were treated with expired medications or none at all, while white inmates received timely care. This segregation extended to mental health, where Black inmates with psychological conditions were frequently isolated or punished rather than treated, exacerbating their suffering.
Practical steps to address this historical injustice today include auditing modern prison healthcare systems for racial disparities and ensuring equitable access to medical care. Advocates must push for transparency in prison health data, particularly regarding treatment outcomes for Black inmates. Additionally, educating the public about this dark chapter in history can foster accountability and prevent its repetition. By dismantling the legacy of Jim Crow in prisons, we can begin to redress the systemic neglect that has persisted for generations.
Transitioning from Army Surgeon to BA Hospital: A Comprehensive Guide
You may want to see also
Explore related products

$2.99 $34

$34.95 $34.95




![]()
Separate and inferior medical facilities for Black patients enforced by Jim Crow legislation
Under Jim Crow laws, Black patients were systematically relegated to separate and substandard medical facilities, a stark manifestation of racial segregation in healthcare. Hospitals designated for Black individuals often operated with inadequate funding, outdated equipment, and a shortage of qualified staff. For instance, in the early 20th century, Black hospitals in the South frequently lacked essential resources like X-ray machines, surgical suites, and even basic sanitation. This disparity was not merely a byproduct of economic inequality but a deliberate policy enforced by state and local governments. The result? Black patients faced higher mortality rates, poorer health outcomes, and limited access to life-saving treatments compared to their white counterparts.
Consider the case of Homer G. Phillips Hospital in St. Louis, one of the few well-equipped Black hospitals in the Jim Crow era. Despite its relative success, it was still underfunded and overburdened, serving a population that had no other options. Meanwhile, white hospitals nearby received significantly more financial support and resources. This pattern repeated across the South, where Black medical facilities were often little more than makeshift clinics, while white hospitals flourished with modern amenities. The segregation extended beyond physical infrastructure to include separate wards, waiting rooms, and even blood supplies, labeled "white" or "colored" to prevent any mixing.
The inferiority of these facilities was not just structural but also operational. Black medical professionals, though highly skilled, were often denied access to training programs and professional networks dominated by whites. This limited their ability to provide advanced care, perpetuating a cycle of substandard treatment for Black patients. For example, Black doctors were rarely allowed to practice in white hospitals, even in emergencies, forcing them to rely on under-resourced institutions. This segregation also meant that Black patients were less likely to receive timely diagnoses or innovative treatments, further entrenching health disparities.
To understand the impact, imagine a Black patient in the 1940s suffering from tuberculosis, a treatable but deadly disease if left unmanaged. While white patients might access sanatoriums with proper ventilation and medication, Black patients were often sent to overcrowded, poorly ventilated wards with limited access to drugs like streptomycin, the era’s breakthrough treatment. This disparity was not accidental but a direct consequence of Jim Crow laws that prioritized white health over Black lives. The legacy of this segregation persists today, with Black communities still facing barriers to quality healthcare.
Addressing this history requires more than acknowledging past injustices. It demands systemic reforms to dismantle the structural inequalities that Jim Crow laws entrenched. Practical steps include increasing funding for historically under-resourced hospitals, diversifying medical education to include more Black professionals, and implementing policies that ensure equitable access to care. By learning from this dark chapter, we can work toward a healthcare system that values all lives equally, regardless of race.
Navigating Evolving Medical Information: A Nurse's Guide to Hospital Management
You may want to see also
Frequently asked questions
Jim Crow laws enforced racial segregation in hospitals, requiring separate facilities for Black and white patients. Black patients often received inferior care, and many hospitals refused to admit them altogether. Black doctors were also excluded from white medical facilities, limiting their ability to practice.
Jim Crow laws perpetuated racial segregation in prisons, with Black and white inmates housed separately. Black prisoners faced harsher treatment, longer sentences, and were often subjected to forced labor, particularly in Southern states. These laws also enabled the disproportionate incarceration of Black individuals through biased policing and judicial practices.
Yes, legal challenges began in the mid-20th century, culminating in landmark cases like *Brown v. Board of Education* (1954) and the Civil Rights Act of 1964, which outlawed segregation in public facilities, including hospitals and prisons. However, the legacy of these laws continues to impact healthcare and the criminal justice system today.