Hospitals in the 1920s were vastly different from their modern counterparts, reflecting the medical knowledge, technology, and societal norms of the era. Characterized by limited antibiotics, rudimentary surgical techniques, and a lack of advanced diagnostic tools, these institutions often focused on basic care and isolation of infectious diseases. Wards were typically large, open spaces with rows of beds, offering little privacy, while nursing care was labor-intensive and relied heavily on manual tasks. The decade also saw the rise of specialized departments, such as obstetrics and pediatrics, and the beginnings of public health initiatives to combat widespread illnesses like tuberculosis. Despite their limitations, 1920s hospitals laid the groundwork for advancements in medicine and healthcare infrastructure in the decades to come.
| Characteristics | Values |
|---|---|
| Medical Technology | Limited; X-rays were common, but advanced machinery like MRI/CT scans were non-existent. Basic surgical tools and anesthesia were used. |
| Hygiene Practices | Poor by modern standards; sterilization was rudimentary, and infections were common. Open wards with minimal privacy. |
| Patient Care | Focused on basic treatment; nursing care was hands-on but with fewer specialized roles. Patients often stayed longer due to slower recovery methods. |
| Hospital Design | Large, open wards with rows of beds; minimal privacy. Often overcrowded and poorly ventilated. |
| Medical Staff | Doctors and nurses were the primary caregivers; specialized roles were rare. Male-dominated profession, especially in surgery. |
| Medications | Limited pharmaceutical options; many treatments were based on natural remedies or early synthetic drugs. Antibiotics were not widely available until later. |
| Surgical Procedures | High-risk due to lack of advanced techniques and infection control. Surgeries were often performed in non-sterile environments. |
| Patient Demographics | Hospitals primarily served the middle and upper classes; poorer populations often relied on home remedies or charity care. |
| Record-Keeping | Manual, paper-based systems; limited data tracking compared to modern electronic health records. |
| Public Health Focus | Emerging focus on infectious disease control, but sanitation and prevention were still developing. |
| Cost of Care | Relatively affordable for the time, but often paid out-of-pocket. Insurance systems were in their infancy. |
| Research and Innovation | Limited; medical research was less institutionalized, and discoveries were slower to translate into practice. |
| Patient Comfort | Minimal; hospitals were utilitarian, with little emphasis on patient comfort or experience. |
| Specialization | General practice dominated; specialized fields like cardiology or neurology were in early stages of development. |
| Emergency Care | Basic and often delayed; no standardized emergency response systems like ambulances or ER protocols. |
Explore related products






What You'll Learn
- Sanitation Practices: Limited hygiene, open wards, shared facilities, and basic disinfection methods were common in hospitals
- Medical Technology: X-rays, early anesthesia, and rudimentary surgical tools were the primary advancements
- Nursing Care: Nurses wore uniforms, worked long hours, and focused on patient comfort and basic care
- Disease Treatment: Focus on tuberculosis, influenza, and pneumonia with limited antibiotics or vaccines
- Hospital Design: Large, airy wards, minimal privacy, and emphasis on natural light and ventilation
![]()
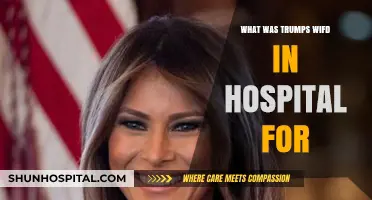
Sanitation Practices: Limited hygiene, open wards, shared facilities, and basic disinfection methods were common in hospitals
In the 1920s, hospitals often struggled with limited hygiene practices, which significantly impacted patient care and recovery. Unlike modern facilities, where stringent cleanliness protocols are standard, hospitals of this era lacked the resources and knowledge to maintain high sanitation levels. Basic necessities like running water and soap were not always readily available, making it difficult for staff to perform frequent handwashing or clean patient areas effectively. This deficiency in hygiene contributed to the spread of infections, as medical professionals often moved between patients without proper sanitization, inadvertently transferring pathogens. The concept of infection control was still in its infancy, and the importance of personal cleanliness in healthcare settings was not yet fully understood or prioritized.
Open wards were a defining feature of 1920s hospitals, further exacerbating sanitation challenges. These large, undivided spaces housed multiple patients with various ailments, from minor injuries to severe illnesses. The lack of privacy and separation meant that contagious diseases could spread rapidly, as there were no barriers to prevent airborne or contact transmission. Patients with infectious conditions were often placed alongside those recovering from surgeries or other treatments, increasing the risk of cross-contamination. The open-ward design, while practical for staff monitoring, created an environment where maintaining cleanliness was nearly impossible, as dust, dirt, and pathogens circulated freely.
Shared facilities were another common aspect of hospital life in the 1920s, adding to the sanitation difficulties. Bathrooms, washbasins, and even bedding were often used by multiple patients, with minimal cleaning in between. Linens were washed infrequently due to limited resources, and reusable items like bedpans and utensils were sometimes rinsed hastily rather than thoroughly disinfected. This shared usage of facilities not only increased the risk of infection but also made it challenging to trace the source of outbreaks. The lack of dedicated, single-patient resources meant that even basic sanitation measures were often compromised, leaving patients vulnerable to hospital-acquired illnesses.
Disinfection methods in 1920s hospitals were rudimentary compared to today’s standards, relying heavily on basic chemicals and manual labor. Common disinfectants included carbolic acid, formaldehyde, and lysol, which were used to clean surfaces and medical instruments. However, these substances were often applied inconsistently, and their effectiveness varied widely. Sterilization of surgical tools was typically achieved through boiling or exposure to heat, methods that were time-consuming and not always reliable. Additionally, the understanding of how to properly disinfect different materials and environments was limited, leading to inadequate sanitation practices. This reliance on basic disinfection techniques meant that hospitals often failed to eliminate harmful pathogens, contributing to higher infection rates among patients and staff.
Despite these challenges, the 1920s marked a transitional period in hospital sanitation, as advancements in medical science began to highlight the importance of cleanliness. Early research on bacteria and infection control started to influence hospital practices, though implementation was slow and uneven. Some progressive institutions began adopting stricter hygiene protocols, such as more frequent cleaning of wards and improved staff training on sanitation. However, these changes were not widespread, and many hospitals continued to operate under outdated practices. The limitations in sanitation during this era underscore the significant strides made in the decades that followed, as healthcare systems gradually prioritized cleanliness and infection prevention.
Tumor Specimen Preservation: Techniques and Hospital Protocols
You may want to see also
Explore related products






![]()
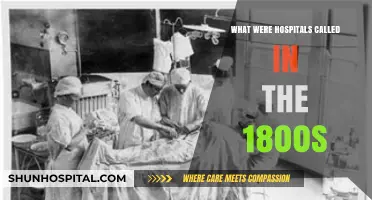
Medical Technology: X-rays, early anesthesia, and rudimentary surgical tools were the primary advancements
In the 1920s, hospitals were undergoing significant transformations, largely driven by advancements in medical technology. Among the most pivotal innovations were X-rays, early anesthesia, and rudimentary surgical tools, which revolutionized diagnostics and treatment. X-rays, discovered in 1895, had become a cornerstone of medical imaging by the 1920s. They allowed physicians to visualize fractures, tumors, and foreign objects inside the body without invasive procedures. However, the technology was still in its infancy; X-ray machines were bulky, required long exposure times, and posed radiation risks due to limited safety protocols. Despite these challenges, X-rays were indispensable in emergency rooms and surgical planning, marking a leap forward in diagnostic accuracy.
Early anesthesia was another critical advancement that shaped hospital care in the 1920s. While anesthesia had been used since the mid-19th century, its application became more refined during this period. Ether and chloroform were the primary anesthetics, administered via drop masks or open-drop techniques. However, anesthesia was not without risks; complications like respiratory depression and allergic reactions were common due to the lack of precise monitoring equipment. Anesthetists relied heavily on clinical observation and experience, as modern ventilators and vital sign monitors did not yet exist. Despite these limitations, anesthesia enabled more complex surgeries, reducing patient pain and mortality rates.
Surgical tools in the 1920s were rudimentary compared to modern standards but represented significant progress from earlier decades. Instruments were primarily made of steel and sterilized using autoclaves, which were becoming more widespread. However, single-use tools were rare, and cross-contamination remained a concern. Surgeons relied on basic instruments like scalpels, forceps, and sutures, often performing procedures under harsh lighting conditions. The introduction of electric cautery tools helped control bleeding, but many surgeries were still risky due to limited understanding of infection control and blood transfusion techniques. Operating rooms were simpler, with tiled walls and minimal equipment, reflecting the era's focus on functionality over sophistication.
The integration of these technologies into hospital settings was gradual and uneven. Urban hospitals were more likely to adopt X-rays and advanced surgical tools, while rural facilities often lagged due to cost and accessibility. Despite these disparities, the 1920s marked a turning point in medical care, as these advancements laid the groundwork for modern medicine. X-rays, anesthesia, and surgical tools not only improved patient outcomes but also expanded the scope of medical interventions, setting the stage for further innovation in the decades to come.
In conclusion, the 1920s were a transformative era for hospitals, defined by the adoption of X-rays, early anesthesia, and rudimentary surgical tools. These technologies, though primitive by today's standards, were revolutionary at the time, enhancing diagnostic capabilities and surgical precision. They also highlighted the challenges of the era, from radiation risks to anesthesia complications, underscoring the ongoing need for medical progress. Together, these advancements shaped the hospital environment, making it a more effective and safer place for patient care.
Hospital Receptionists: The Face and Heart of Patient Care
You may want to see also
Explore related products






![]()
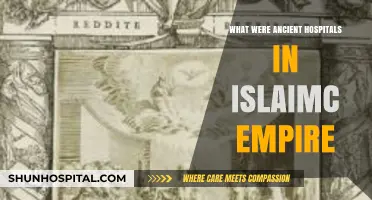
Nursing Care: Nurses wore uniforms, worked long hours, and focused on patient comfort and basic care
In the 1920s, nursing care was a cornerstone of hospital operations, characterized by dedication, discipline, and a strong emphasis on patient comfort. Nurses were easily identifiable by their uniforms, which typically consisted of starched white dresses, aprons, and caps. These uniforms symbolized cleanliness and professionalism, reflecting the high standards expected of nursing staff. The attire was not just about appearance; it also served practical purposes, such as protecting the nurse’s clothing and maintaining hygiene in a clinical setting. The uniform was a badge of honor, signifying the nurse’s role as a caregiver and a trusted member of the healthcare team.
Nurses in the 1920s worked long, demanding hours, often with minimal breaks. Twelve-hour shifts were common, and many nurses lived on-site in hospital dormitories to ensure they were always available. This dedication came at a personal cost, as it left little time for rest or personal life. Despite the challenges, nurses took pride in their work, viewing their role as a calling rather than just a job. Their commitment was driven by a sense of duty to their patients and a desire to provide the best possible care under often difficult circumstances.
Patient comfort was a primary focus of nursing care in the 1920s. Hospitals were not yet equipped with many of the modern conveniences we take for granted today, so nurses relied on hands-on care to ensure patients were as comfortable as possible. This included tasks like adjusting bed linens, providing warm blankets, and assisting with personal hygiene. Nurses also played a crucial role in monitoring patients’ conditions, administering medications, and assisting doctors during procedures. Their presence was a source of reassurance for patients, many of whom were hospitalized for extended periods due to the limitations of medical technology at the time.
Basic care was another key aspect of nursing in the 1920s, as hospitals lacked the advanced equipment and treatments available today. Nurses often had to improvise, using simple tools and techniques to address patients’ needs. For example, they might use hot water bottles to relieve pain or hand-feed patients who were too weak to eat on their own. This hands-on approach required patience, creativity, and a deep understanding of human needs. Nurses were not just caregivers; they were also advocates, ensuring that patients received the attention and support they needed to recover.
The role of nurses in the 1920s extended beyond physical care to emotional and psychological support. Hospitals could be intimidating and isolating places, especially for long-term patients. Nurses often spent time talking to patients, listening to their concerns, and offering words of encouragement. This compassionate approach was a vital part of the healing process, helping patients maintain hope and resilience in the face of illness. Through their uniforms, long hours, and focus on comfort and basic care, nurses in the 1920s laid the foundation for the patient-centered care that remains a hallmark of nursing today.
Hospitals and Hair Follicle Drug Testing: What's the Connection?
You may want to see also
Explore related products






![]()
Disease Treatment: Focus on tuberculosis, influenza, and pneumonia with limited antibiotics or vaccines
In the 1920s, hospitals faced significant challenges in treating infectious diseases like tuberculosis, influenza, and pneumonia, primarily due to the limited availability of antibiotics and vaccines. Tuberculosis, often called "consumption," was a leading cause of death and was treated with a combination of rest, fresh air, and a nutritious diet. Sanatoria, specialized hospitals for tuberculosis patients, became widespread. Patients were often placed in open-air wards or on porches, even in cold weather, under the belief that fresh air and sunlight could combat the disease. Surgical interventions, such as the collapse of an infected lung to allow it to heal, were also employed, though these procedures were risky and not always effective.
Influenza, still a major threat following the devastating 1918 pandemic, was treated symptomatically, as no effective antiviral medications or vaccines were available. Hospitals focused on providing supportive care, such as hydration, rest, and medications to reduce fever and alleviate pain. Aspirin was commonly used, though its overuse sometimes led to complications. Quarantine measures were also implemented to limit the spread of the virus, but these were often insufficient in densely populated areas. The lack of understanding about viral transmission meant that preventive measures were rudimentary compared to modern standards.
Pneumonia, frequently a secondary infection following influenza or tuberculosis, was another major concern. Without antibiotics, treatment relied on bed rest, fluid intake, and oxygen therapy when available. Physicians sometimes used crude methods like bloodletting or the application of poultices, though these were largely ineffective. The mortality rate for pneumonia remained high, particularly among the elderly, children, and those with weakened immune systems. Hospitals often isolated pneumonia patients to prevent the spread of the disease, but overcrowding and poor sanitation in many facilities exacerbated the problem.
The limited availability of antibiotics in the 1920s meant that bacterial infections, including those associated with tuberculosis and pneumonia, were often fatal. Sulfonamides, the first widely used antibacterial agents, would not be discovered until the 1930s, and penicillin would not become available until the 1940s. As a result, physicians relied on experimental treatments, such as the use of colloidal silver or injections of vaccines derived from bacterial cultures, with varying degrees of success. Surgery was sometimes performed to drain abscesses or remove infected tissue, but these procedures carried significant risks due to the lack of effective anesthesia and sterile techniques.
Despite these challenges, the 1920s saw advancements in hospital care that laid the groundwork for future improvements. Public health campaigns emphasized hygiene and sanitation to prevent the spread of disease, and hospitals began to adopt more systematic approaches to patient care. Research into the causes and treatments of tuberculosis, influenza, and pneumonia intensified, driven by the high mortality rates associated with these diseases. While the treatments available in the 1920s were often inadequate by modern standards, they reflected the best medical knowledge of the time and the determination of healthcare providers to combat these devastating illnesses.
Trauma Center Levels: Understanding Hospital Capabilities
You may want to see also
Explore related products




![The Hospital [DVD]](https://m.media-amazon.com/images/I/61oQ2sBPcmL._AC_UY218_.jpg)

![]()
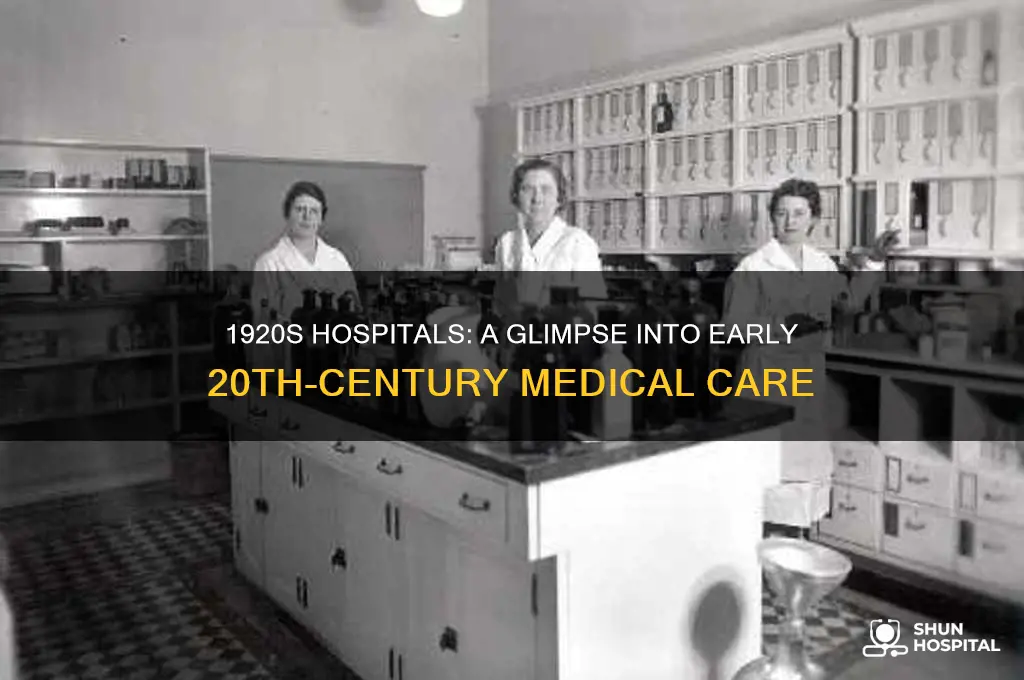
Hospital Design: Large, airy wards, minimal privacy, and emphasis on natural light and ventilation
In the 1920s, hospital design underwent significant transformations, reflecting the era's understanding of hygiene, patient care, and medical advancements. Large, airy wards were a hallmark of this period, designed to accommodate multiple patients in a single space. These wards often featured high ceilings and expansive windows, creating an open environment that facilitated the circulation of fresh air. The layout was not only practical for nursing staff, who could monitor numerous patients at once, but also aligned with the prevailing belief that fresh air was therapeutic. This design philosophy was rooted in the pre-antibiotic era, where ventilation was considered a critical factor in preventing the spread of infections.
Minimal privacy was another characteristic of 1920s hospital wards. Patients were often separated by simple curtains or low partitions, if at all. This lack of privacy was both a result of the era's communal approach to healthcare and the practicalities of managing large numbers of patients with limited resources. The focus was on efficiency and accessibility rather than individual comfort. Nurses and doctors could move freely through the wards, providing care without the barriers of private rooms. This open layout also fostered a sense of community among patients, though it came at the expense of personal space and confidentiality.
Natural light played a pivotal role in hospital design during this period. Large windows were strategically placed to maximize daylight, reducing the reliance on artificial lighting and creating a brighter, more uplifting environment. Sunlight was believed to have healing properties, particularly for conditions like tuberculosis, which was prevalent at the time. The emphasis on natural light also improved visibility for medical staff, making it easier to perform tasks and observe patients. This design element was not just functional but also psychological, as it helped combat the sterile and often intimidating atmosphere of hospitals.
Ventilation was a cornerstone of 1920s hospital architecture, driven by the era's focus on infection control. Wards were designed with cross-ventilation in mind, often featuring windows on opposite walls to allow air to flow freely. Some hospitals even incorporated advanced systems like night ventilation, where windows were slightly opened during cooler night hours to refresh the air without causing discomfort. The use of materials like linoleum flooring and washable walls further supported hygiene efforts, as they were easy to clean and resistant to bacteria. This attention to airflow and cleanliness was a direct response to the high mortality rates associated with hospital-acquired infections in earlier decades.
In summary, the hospital design of the 1920s was characterized by large, airy wards, minimal privacy, and a strong emphasis on natural light and ventilation. These features reflected the era's medical priorities, blending practicality with the therapeutic benefits of light and fresh air. While the lack of privacy and communal nature of these wards may seem outdated by today's standards, they were innovative solutions to the challenges of the time, shaping the evolution of healthcare environments in the decades that followed.
Parents in Hospital: Who's Allowed Inside?
You may want to see also
Frequently asked questions
Hospitals in the 1920s had limited medical technology compared to today. X-ray machines were becoming more common, but other advanced equipment like MRI or CT scanners did not exist. Surgical tools were basic, and anesthesia was primarily ether or chloroform. Antibiotics were not yet widely available, making infections a significant risk.
Hospitals in the 1920s relied heavily on nurses, who often worked long hours with minimal staff. Doctors were typically general practitioners, as specialization was less common. Many hospitals also employed orderlies and cleaning staff, but roles were often gender-segregated, with women dominating nursing and men in administrative or maintenance roles.
Patient conditions varied widely. Urban hospitals were often overcrowded, with shared wards and limited privacy. Rural hospitals were smaller and had fewer resources. Sanitation was improving but still a concern, and infections were common. Patients often stayed longer due to slower recovery times and limited treatment options.
Hospitals in the 1920s were still recovering from the 1918 flu pandemic, which had overwhelmed many facilities. Efforts focused on quarantine, basic hygiene, and supportive care, as antiviral medications did not exist. Public health campaigns emphasized prevention, but hospitals remained critical for treating severe cases and managing outbreaks.