Hospitals in the past were vastly different from the modern, technologically advanced institutions we know today. Historically, these facilities often served as places of last resort, primarily catering to the poor, the elderly, and the incurably ill. In ancient civilizations like Egypt and Greece, healing temples combined spiritual rituals with rudimentary medical care, while medieval European hospitals were frequently run by religious orders, focusing on providing shelter and spiritual comfort rather than advanced treatments. During the Renaissance and Enlightenment periods, hospitals began to evolve, with the emergence of early surgical practices and the separation of patients by ailment, though sanitation and patient outcomes remained poor by contemporary standards. The Industrial Revolution brought further changes, as urbanization and medical advancements led to more specialized care, laying the groundwork for the modern hospital system.
Explore related products






What You'll Learn
![]()
Ancient Civilizations' Healing Centers
In the ancient world, healing centers were often deeply intertwined with religious and spiritual practices, reflecting the belief that illnesses were caused by supernatural forces or imbalances in the body. Ancient Egyptian healing centers, for example, were closely associated with temples dedicated to gods like Imhotep, the deity of medicine. These centers, known as "per-ankh" or "house of life," were places where priests, who also served as physicians, practiced medicine. They treated ailments through a combination of herbal remedies, surgical procedures, and magical incantations. The Ebers Papyrus, an ancient Egyptian medical text, reveals their advanced knowledge of anatomy, diagnostics, and treatments, including remedies for wounds, skin conditions, and even dental issues. Patients would often undergo rituals to appease the gods as part of their healing process.
Mesopotamian healing centers similarly blended medicine with spirituality, as evidenced by clay tablets from ancient Sumer and Babylon. These centers were called "bēt šāritim" or "house of the healer," where trained physicians, known as "asû," diagnosed illnesses by examining symptoms and interpreting omens. Treatments included herbal medicines, bandaging, and even early forms of psychotherapy. The Code of Hammurabi, a Babylonian legal text, regulated medical practice, imposing penalties for malpractice. Healing centers were often attached to temples, and physicians relied on both empirical observation and religious rituals to cure patients, reflecting the belief that diseases were punishments from the gods.
Ancient Greek healing centers, known as "asclepieia," were dedicated to Asclepius, the god of medicine. These sanctuaries were places of pilgrimage where patients would sleep in special areas to receive healing dreams or visions from the god. The process, called "incubation," involved rituals, prayers, and offerings. Priests and physician-healers would interpret these dreams and prescribe treatments, which often included diet, exercise, and herbal remedies. The asclepieia also emphasized the importance of hygiene and a healthy lifestyle, principles later developed by physicians like Hippocrates, who is often regarded as the father of Western medicine. These centers were among the first to separate medicine from religion, focusing more on natural causes of illness.
Ancient Indian healing centers, rooted in Ayurvedic traditions, were holistic institutions that treated the body, mind, and spirit as interconnected. Ayurvedic hospitals, often attached to monasteries or royal courts, used natural remedies, yoga, meditation, and dietary adjustments to restore balance in the body's doshas (humors). Physicians, known as "vaidyas," were highly trained and relied on texts like the Charaka Samhita and Sushruta Samhita, which detailed surgical techniques, herbal treatments, and preventive care. These centers also emphasized the role of environment and lifestyle in health, advocating for clean living spaces and ethical behavior as part of the healing process.
Ancient Roman healing centers evolved from Greek influences but were more secular and practical. Roman hospitals, called "valetudinaria," were primarily established to treat soldiers and slaves. These institutions were among the first to focus on public health, with organized wards, surgical tools, and recovery areas. Roman physicians like Galen made significant contributions to anatomy and surgery, and their hospitals often included pharmacies and dietary programs. While less spiritual than their predecessors, Roman healing centers laid the groundwork for modern medical institutions by emphasizing systematic care and the importance of trained medical professionals.
Navigating to NKS Hospital: Easy Access Guide
You may want to see also
Explore related products





![]()
Medieval European Hospices
In the context of Medieval Europe, hospices played a crucial role in providing care for the sick, poor, and travelers. These institutions, often established by the Church or wealthy patrons, were not merely places for medical treatment but also served as centers for spiritual and charitable work. Medieval European hospices were typically attached to monasteries, convents, or cathedrals, reflecting the deep intertwining of religion and healthcare during this period. The primary goal was to offer solace, comfort, and basic care rather than advanced medical interventions, as the understanding of medicine was limited compared to modern standards.
The physical structure of medieval hospices varied, but they were generally simple and functional. Most were modest buildings with dormitories for patients, a chapel for prayers, and a refectory for meals. Hygiene was a significant challenge, as the concept of germ theory was unknown, and sanitation practices were rudimentary. Patients often shared beds, and the lack of proper ventilation and cleanliness contributed to the spread of infections. Despite these limitations, hospices were considered sanctuaries for those in need, providing a rare haven for the afflicted in a time when societal support systems were scarce.
The staff of these hospices consisted mainly of monks, nuns, and lay volunteers who were motivated by religious duty and compassion. Medical knowledge was rudimentary, and treatments were often based on herbal remedies, prayer, and rest. Bloodletting, a common practice at the time, was also employed, though its effectiveness was questionable. The caregivers focused on alleviating suffering rather than curing diseases, as many ailments were beyond the scope of medieval medicine. Spiritual care was equally important, with daily prayers and sacraments being a central part of the hospice routine.
Funding for medieval hospices came from various sources, including donations from the wealthy, tithes from the Church, and endowments from charitable individuals. These institutions relied heavily on the generosity of the community, as there was no centralized healthcare system. Pilgrims and travelers often contributed to the upkeep of hospices, as they were frequent beneficiaries of their services. The charitable nature of these establishments ensured their survival, even in times of economic hardship, as they were seen as essential for the moral and spiritual well-being of society.
In summary, medieval European hospices were vital institutions that combined healthcare, spirituality, and charity. While they lacked the medical sophistication of modern hospitals, they provided a compassionate and supportive environment for the vulnerable. Their legacy highlights the enduring human need for care and the historical intersection of religion and medicine. Understanding these early forms of healthcare sheds light on the evolution of hospitals and the enduring importance of compassion in medical practice.
The Heart of Hospitality: Defining Service Excellence
You may want to see also
Explore related products






![]()
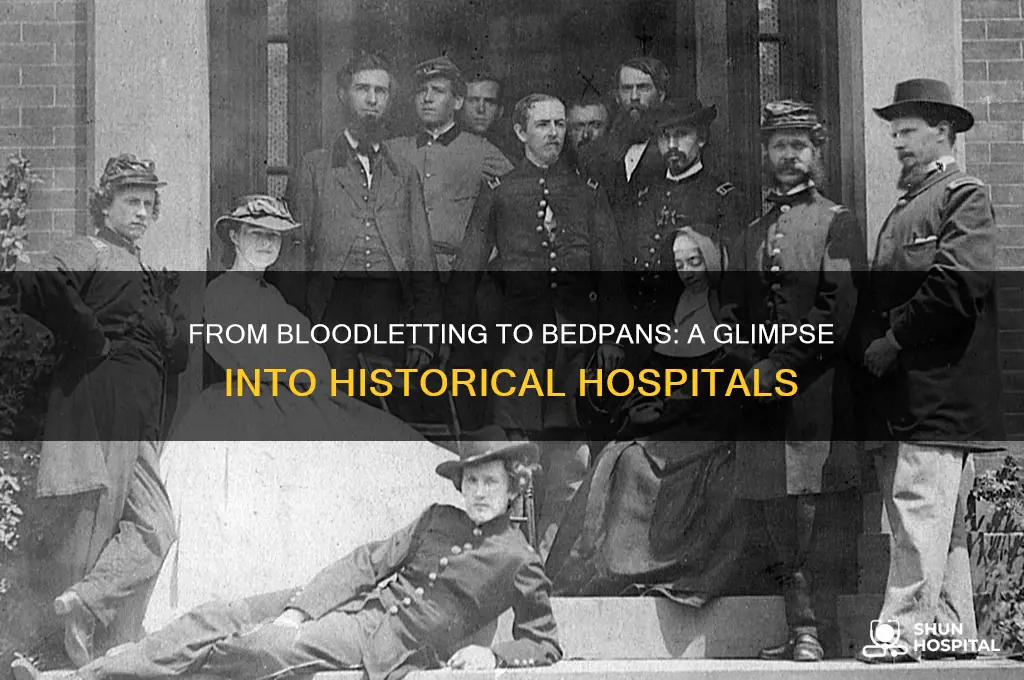
Military Field Hospitals
During the American Civil War (1861–1865), military field hospitals saw some improvements but remained primitive by today’s standards. Hospitals were often set up in barns, churches, or private homes, with little regard for hygiene. Medical supplies were scarce, and anesthesia, though available, was inconsistently administered. Nurses, often volunteers or soldiers’ wives, worked tirelessly under grueling conditions, lacking formal training. The triage system began to take shape, with wounded soldiers categorized by the severity of their injuries, but resources were insufficient to meet the demand. The lack of proper transportation also meant that many soldiers died before reaching medical care, as ambulances were horse-drawn and slow.
By World War I (1914–1918), military field hospitals had evolved significantly, though they still faced immense challenges. The introduction of motorized ambulances and railway transport allowed for quicker evacuation of the wounded. Hospitals were better organized, with designated wards for surgery, recovery, and infectious diseases. However, the scale of casualties from trench warfare and new weapons like machine guns and chemical agents overwhelmed these facilities. Surgeons performed countless amputations and treated horrific injuries, often working in dimly lit, overcrowded tents or makeshift buildings. Despite advancements in anesthesia and the introduction of blood transfusions, infection remained a leading cause of death due to the prevalence of antibiotic-resistant bacteria.
World War II (1939–1945) marked a turning point for military field hospitals, with greater emphasis on mobility, sanitation, and specialization. Mobile Army Surgical Hospitals (MASH units) became iconic, providing rapid, frontline care to stabilize soldiers before they were evacuated to larger facilities. These hospitals were equipped with X-ray machines, blood banks, and rudimentary surgical suites. The introduction of penicillin revolutionized infection treatment, drastically reducing mortality rates. However, conditions were still harsh, with surgeons operating in tents or bombed-out buildings, often under enemy fire. The psychological toll on medical personnel was immense, as they faced constant streams of wounded soldiers and the moral dilemmas of triage.
In summary, military field hospitals of the past were defined by their adaptability, resourcefulness, and the relentless efforts of medical personnel under extreme conditions. From the unsanitary tents of the Crimean War to the mobile, specialized units of World War II, these hospitals evolved in response to the changing nature of warfare and medical science. Despite their limitations, they played a crucial role in saving lives and laid the foundation for modern military medicine. Their legacy is a testament to human resilience and the enduring mission to heal, even in the midst of chaos.
Eye and Ear Hospital: Free or Fee?
You may want to see also
Explore related products






![]()
19th Century Asylums
In the 19th century, asylums were a stark reflection of societal attitudes toward mental illness, often characterized by neglect, overcrowding, and inhumane treatment. These institutions emerged as a response to the growing recognition of mental health issues, but they were far from the therapeutic environments we envision today. Asylums during this period were typically large, imposing structures, designed to house and control rather than heal. The architecture itself was a statement of isolation, with high walls and barred windows, symbolizing the separation of the "insane" from the rest of society. Patients were often admitted against their will, and once inside, they faced a rigid and dehumanizing routine.
The conditions within 19th-century asylums were appalling by modern standards. Overcrowding was a pervasive issue, with facilities frequently housing far more patients than they were designed to accommodate. This led to unsanitary living conditions, as basic hygiene and cleanliness were often neglected. Patients were often grouped together regardless of their specific conditions, leading to a chaotic and stressful environment. The lack of individualized care meant that many patients received little to no treatment, and the focus was more on containment than recovery. Physical restraints, such as straitjackets and manacles, were commonly used to control patients, further exacerbating their distress.
Staffing in these asylums was another critical issue. The caregivers were often poorly trained and overworked, leading to a lack of empathy and understanding for the patients' needs. The role of the asylum superintendent was typically filled by a physician, but their primary focus was on administration rather than patient care. Nurses and attendants, who had the most direct contact with patients, were frequently underpaid and undertrained, resulting in a cycle of abuse and neglect. The power dynamics within these institutions often led to mistreatment, with patients having little to no rights or recourse against their caretakers.
Treatment methods in 19th-century asylums were rudimentary and often based on flawed theories of mental illness. Bloodletting, purging, and the use of mercury were common practices, reflecting the era's limited understanding of mental health. The introduction of moral treatment, advocated by reformers like Philippe Pinel and William Tuke, offered a more humane approach, emphasizing kindness, structured activities, and a supportive environment. However, this philosophy was not widely adopted, and many asylums continued to rely on harsh, punitive measures. The use of isolation cells, cold baths, and even physical punishment was not uncommon, further traumatizing patients.
Despite the grim reality of 19th-century asylums, this period also saw the beginnings of reform efforts. Social reformers and pioneering psychiatrists began to advocate for better conditions and more compassionate care. The work of individuals like Dorothea Dix in the United States played a crucial role in exposing the horrors of asylums and pushing for legislative changes. Her efforts led to increased funding and the establishment of new institutions with a greater emphasis on patient welfare. However, these reforms were gradual, and it would take many decades for significant improvements to be realized in the care and treatment of the mentally ill.
In conclusion, 19th-century asylums were institutions marked by harsh conditions, inadequate care, and a profound lack of understanding of mental health. While they represented an early attempt to address the needs of the mentally ill, they often caused more harm than good. The legacy of these asylums serves as a reminder of the importance of compassionate, evidence-based care and the ongoing need for reform in mental health treatment. The struggles and suffering of patients during this era highlight the critical importance of human dignity and individualized care in any healthcare setting.
Who Qualifies for VA Hospital Care: Eligibility and Patient Acceptance
You may want to see also
Explore related products






![]()
Early 20th Century Sanatoria
In the early 20th century, sanatoria played a unique and critical role in healthcare, primarily as specialized institutions for the treatment of tuberculosis (TB), a widespread and often fatal disease at the time. Unlike general hospitals, sanatoria were designed to provide long-term care in environments that emphasized fresh air, sunlight, and rest—principles rooted in the pre-antibiotic era's understanding of TB treatment. These facilities were often located in rural or mountainous areas, where the clean air was believed to aid recovery. Patients would spend months or even years in sanatoria, following strict regimens that included outdoor exposure, controlled diets, and limited physical activity.
The architecture of early 20th-century sanatoria reflected their therapeutic goals. Buildings featured large windows, open balconies, and spacious wards to maximize natural light and ventilation. Many were designed in the style of grand, resort-like structures, with gardens and walking paths to encourage patients to spend time outdoors. The layout was intentional, prioritizing the health benefits of the environment over the clinical efficiency seen in modern hospitals. Despite their serene appearance, these institutions were places of isolation, where patients were often separated from their families for extended periods to prevent the spread of TB.
Life in a sanatorium was highly regimented. Patients adhered to strict schedules that included periods of rest, exercise, and meals. Activities like reading, knitting, or painting were encouraged to keep patients occupied, but physical exertion was minimized to conserve energy. Medical treatments were limited, as effective antibiotics for TB were not yet available. Instead, therapies included procedures like pneumothorax (collapsing a lung to rest the affected area) and the administration of cod liver oil or ultraviolet light. The focus was on managing symptoms and preventing disease progression rather than curing it.
Sanatoria were also social microcosms, housing patients from diverse backgrounds. While some were privately funded and catered to wealthier individuals, others were public institutions serving the working class. This mix of patients often led to a sense of community, as individuals bonded over shared experiences of illness and isolation. However, the atmosphere could also be bleak, as the mortality rate for TB remained high, and many patients faced uncertain futures. The emotional toll of prolonged separation from loved ones and the constant presence of death made sanatoria places of both hope and despair.
By the mid-20th century, the role of sanatoria began to decline with the advent of antibiotics like streptomycin, which revolutionized TB treatment. The need for long-term, environment-focused care diminished as patients could be treated more effectively on an outpatient basis. Many sanatoria were repurposed into general hospitals or closed entirely, marking the end of an era in medical history. Despite their eventual obsolescence, early 20th-century sanatoria remain a testament to the ingenuity and limitations of pre-modern medicine, offering insights into how societies once approached the treatment of chronic and deadly diseases.
Austin's Top-Tier Hospitals: A Comprehensive Overview
You may want to see also
Frequently asked questions
Hospitals in ancient civilizations, such as those in Egypt, Greece, and Rome, were often tied to religious or spiritual practices. They were basic in structure, with limited medical knowledge, and relied heavily on herbal remedies, prayers, and rituals. Facilities were often attached to temples, and care was provided by priests or early physicians like Hippocrates.
Medieval hospitals were primarily run by the Church and focused on providing charity and spiritual care rather than advanced medical treatment. They served the poor, pilgrims, and the sick, offering basic shelter, food, and prayers. Surgical procedures were rare, and medical practices were often based on humorism and bloodletting.
Hospitals in the 19th century began to modernize with advancements in medical science and sanitation. They became more focused on curing diseases rather than just providing shelter. The introduction of anesthesia, antiseptic techniques, and nursing practices (thanks to figures like Florence Nightingale) significantly improved patient care. However, overcrowding and poor hygiene were still common issues.