In the context of disaster preparedness, the Emergency Department (ED) of a hospital typically plays the primary role due to its critical function in immediate response and triage during crises. However, effective disaster preparedness is a multidisciplinary effort, involving collaboration across various departments. The ED leads in frontline care, while other departments such as Administration, Infection Control, Pharmacy, and Facilities Management contribute by ensuring resource allocation, infection prevention, medication supply, and infrastructure integrity. Together, these departments form a cohesive network to enhance resilience and response capabilities in the face of disasters.
Explore related products






What You'll Learn
- Emergency Department: Triage, treatment, and coordination during disasters
- Public Health: Disease prevention, surveillance, and community health protection
- Administration: Resource allocation, policy implementation, and hospital-wide coordination
- Trauma Services: Specialized care for mass casualty incidents and injuries
- Logistics: Supply chain management, equipment readiness, and facility preparedness
![]()
Emergency Department: Triage, treatment, and coordination during disasters
In the chaotic aftermath of a disaster, the Emergency Department (ED) becomes the epicenter of medical response, a critical hub where lives hang in the balance. The ED's primary role is to swiftly assess, treat, and coordinate care for a sudden influx of patients, many with critical or complex injuries. This demands a highly structured yet adaptable approach, centered on triage, treatment, and coordination.
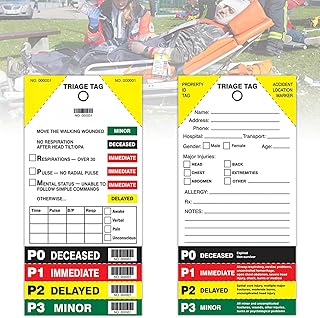
Triage, the initial sorting of patients based on severity, is the linchpin of disaster response in the ED. Utilizing systems like START (Simple Triage and Rapid Treatment) or SALT (Sort, Assess, Lifesaving Interventions, Treatment/Transport), trained personnel rapidly categorize patients into groups: immediate (red), delayed (yellow), minor (green), and deceased (black). This ensures those most critically injured receive immediate attention, maximizing survival rates. For instance, a patient with severe bleeding and a weak pulse would be triaged as red, requiring immediate intervention like tourniquets, fluid resuscitation, and potential surgery.
A well-organized treatment plan within the ED is crucial. This involves setting up designated areas for different levels of care, from critical care bays for the most severe cases to observation areas for those requiring monitoring but not immediate intervention. Treatment protocols must be streamlined and adaptable, focusing on stabilizing patients and preventing further deterioration. For example, during a mass casualty incident involving burns, the ED might establish a dedicated burn unit with specialized personnel and equipment, including burn dressings, intravenous fluids, and pain management protocols.
Effective coordination is the glue that holds the ED's disaster response together. This involves seamless communication between ED staff, hospital administration, emergency medical services, and external agencies. Clear lines of authority and designated roles are essential to prevent confusion and ensure efficient resource allocation. For instance, a designated incident commander oversees the overall response, while liaison officers coordinate with external agencies for additional resources like blood supplies or specialized medical teams.
The ED's role in disaster preparedness extends beyond the immediate response. Regular drills and simulations are vital to test protocols, identify weaknesses, and train staff. These exercises should incorporate realistic scenarios, including mass casualty incidents, chemical spills, or pandemics. Additionally, maintaining adequate supplies of essential medications, equipment, and personal protective gear is crucial for sustained response capabilities.
In essence, the Emergency Department serves as the frontline in disaster preparedness, a dynamic and challenging environment where triage, treatment, and coordination converge to save lives. Its success relies on meticulous planning, skilled personnel, and a commitment to continuous improvement, ensuring readiness to face the unpredictable nature of disasters.
Good Samaritan Hospital Distance from Hammond, NY: A Quick Guide
You may want to see also
Explore related products






![]()
Public Health: Disease prevention, surveillance, and community health protection
Public health departments are the backbone of disease prevention and community health protection during disasters, often operating in the shadows of more visible emergency response teams. Their primary role is to anticipate, detect, and mitigate health threats before they escalate into crises. For instance, during a hurricane, public health teams might pre-position vaccines and antibiotics in shelters, ensuring that displaced populations are protected against outbreaks of vaccine-preventable diseases like influenza or hepatitis A. This proactive approach is critical, as disasters disrupt healthcare systems, making routine immunizations and disease surveillance nearly impossible.
Surveillance is another cornerstone of public health’s disaster preparedness efforts. By monitoring disease trends in real-time, these departments can identify outbreaks early and respond swiftly. For example, after a flood, public health officials test water sources for contaminants like E. coli and cholera, issuing boil-water advisories if necessary. They also track increases in vector-borne diseases like West Nile virus or dengue fever, which thrive in standing water. This data-driven approach allows for targeted interventions, such as mosquito control programs or public education campaigns on avoiding bites.
Community health protection extends beyond immediate disease threats to address long-term health impacts of disasters. Public health teams educate communities on preventing mold-related illnesses after floods, recommending the use of N95 masks during cleanup and advising on proper ventilation techniques. They also provide mental health resources, recognizing that disasters often lead to increased rates of anxiety, depression, and PTSD. For vulnerable populations, such as the elderly or immunocompromised, public health departments may offer tailored guidance, like ensuring a 30-day supply of medications or providing access to cooling centers during heatwaves.
A critical yet often overlooked aspect of public health’s role is its collaboration with other hospital departments and external agencies. For instance, during a wildfire, public health officials work with emergency departments to manage an influx of patients with respiratory issues, ensuring adequate supplies of bronchodilators like albuterol. They also coordinate with environmental health agencies to monitor air quality, advising the public to stay indoors when particulate matter levels exceed 300 µg/m³. This interdisciplinary approach ensures a holistic response, addressing both immediate and long-term health needs.
Ultimately, the success of disaster preparedness hinges on public health’s ability to act as both a sentinel and a shield. By focusing on disease prevention, surveillance, and community health protection, these departments create resilient communities capable of withstanding and recovering from disasters. Their work is not just about responding to crises but about building systems that minimize health risks before they occur. In a world increasingly vulnerable to natural and man-made disasters, public health’s role has never been more critical.
Crafting a Compelling Art Submission Email for Hospital Displays
You may want to see also
Explore related products


$19.71 $21.99

$14.39 $17.99


![]()
Administration: Resource allocation, policy implementation, and hospital-wide coordination
Effective disaster preparedness in hospitals hinges on the administration’s ability to allocate resources strategically, implement policies seamlessly, and ensure hospital-wide coordination. Without these elements, even the most well-equipped facilities can falter under pressure. Resource allocation, for instance, is not merely about stockpiling supplies but involves a nuanced understanding of demand forecasting, supply chain resilience, and prioritization. During a disaster, the administration must decide whether to allocate 70% of available ventilators to the ICU or distribute them across departments based on patient acuity—a decision that can mean the difference between life and death.
Policy implementation serves as the backbone of disaster response, transforming theoretical plans into actionable protocols. Consider the activation of a surge capacity plan: the administration must ensure that policies for staff redeployment, patient triage, and alternative care sites are not only documented but also practiced and understood by every employee. For example, a hospital in Japan mandates annual drills where administrative staff simulate the activation of their incident command system, reducing response times by 40% during actual emergencies. Such drills highlight the importance of clarity and repetition in policy execution.
Hospital-wide coordination is the glue that binds disparate departments into a cohesive unit during a crisis. The administration must act as the central nervous system, ensuring that the emergency department, pharmacy, and IT services operate in sync. A case study from Hurricane Katrina revealed that hospitals with designated coordination officers experienced 30% fewer logistical delays compared to those without. These officers facilitated real-time communication, resolved resource conflicts, and ensured that critical decisions were relayed swiftly across all levels of the organization.
To optimize administrative preparedness, hospitals should adopt a three-pronged approach: first, conduct regular resource audits to identify gaps and redundancies; second, integrate policy training into staff onboarding and annual refreshers; and third, establish a cross-departmental coordination team with clear roles and communication channels. By doing so, administrations can transform potential chaos into a structured, efficient response. After all, in disaster scenarios, the strength of a hospital’s administration is measured not by its plans on paper but by its ability to execute them under fire.
Texas Hospitals: Can You Carry a Concealed Weapon?
You may want to see also
Explore related products





![]()
Trauma Services: Specialized care for mass casualty incidents and injuries
Trauma services stand as the linchpin in hospital disaster preparedness, particularly during mass casualty incidents (MCIs). These specialized units are designed to handle the unique challenges of MCIs, where the volume and severity of injuries overwhelm standard emergency department (ED) capabilities. Unlike routine trauma cases, MCIs require a coordinated, scalable response that prioritizes rapid triage, resource allocation, and life-saving interventions. Trauma services are equipped with dedicated teams, including trauma surgeons, critical care nurses, and respiratory therapists, who are trained to manage complex, multi-system injuries in high-pressure environments. Their role extends beyond immediate care, encompassing pre-incident planning, surge capacity management, and post-event debriefing to ensure continuous improvement.
Consider the logistical demands of an MCI: a single incident can produce dozens of critically injured patients within minutes. Trauma services employ structured protocols like the START (Simple Triage and Rapid Treatment) system to categorize patients into priority groups—immediate, delayed, minimal, or expectant. This triage method ensures that limited resources are directed to those with the highest survival potential. For instance, a patient with a tension pneumothorax requires immediate needle decompression, while a stable fracture can wait. Trauma teams also rely on pre-established algorithms for interventions such as massive transfusion protocols, which deliver blood products in a 1:1:1 ratio of plasma, platelets, and red cells to manage hemorrhagic shock. These protocols are rehearsed during drills, ensuring seamless execution when real incidents occur.
The physical layout of trauma services is another critical factor. These units often feature resuscitation bays with multiple beds, overhead booms for monitoring equipment, and immediate access to imaging modalities like portable X-ray and ultrasound. For example, the use of focused assessment with sonography for trauma (FAST) allows rapid detection of internal bleeding, guiding immediate interventions. Additionally, trauma services maintain stockpiles of specialized equipment, such as external fixators for pelvic fractures and intraosseous devices for vascular access in pediatric patients (recommended for children under 6 years old due to difficult peripheral access). These resources are not typically available in general EDs, underscoring the unique role of trauma services in disaster response.
A persuasive argument for the centrality of trauma services lies in their ability to reduce mortality rates during MCIs. Studies show that hospitals with Level I or II trauma centers—which include specialized trauma services—achieve significantly better outcomes in MCIs compared to non-trauma centers. For instance, a 2018 analysis of the Boston Marathon bombing response highlighted how trauma-trained teams minimized fatalities through rapid hemorrhage control and airway management. However, this expertise comes with a caveat: trauma services must be integrated into broader hospital and regional disaster plans. Failure to coordinate with other departments, such as surgery or ICU, can lead to bottlenecks in patient flow and resource depletion. Hospitals should conduct regular tabletop exercises to test these integrations, ensuring trauma services function as part of a cohesive system.
In conclusion, trauma services are indispensable in disaster preparedness due to their specialized training, infrastructure, and protocols tailored to MCIs. Their ability to triage, treat, and stabilize large numbers of critically injured patients makes them the primary responders in catastrophic events. Hospitals must invest in these units, not only by equipping them with advanced tools but also by fostering interdisciplinary collaboration and continuous training. By doing so, trauma services can fulfill their mission: to save lives when disaster strikes.
Beaumont Hospital Dearborn: Private or Public?
You may want to see also
Explore related products






![]()
Logistics: Supply chain management, equipment readiness, and facility preparedness
Effective disaster preparedness in hospitals hinges on robust logistics, a multifaceted discipline that ensures the seamless flow of resources, equipment, and operational continuity when every second counts. At its core, supply chain management must anticipate and mitigate disruptions to essential medical supplies, pharmaceuticals, and consumables. For instance, during the COVID-19 pandemic, hospitals faced critical shortages of personal protective equipment (PPE) and ventilators, exposing vulnerabilities in global supply chains. To counter this, hospitals should adopt just-in-case inventory strategies for high-demand items, such as maintaining a 30-day stockpile of PPE and critical medications. Additionally, diversifying suppliers across regions and establishing local manufacturing partnerships can reduce dependency on single sources, ensuring resilience against geopolitical or logistical shocks.
Equipment readiness is another pillar of logistical preparedness, demanding proactive maintenance and strategic deployment. Hospitals must conduct regular audits of life-saving devices like defibrillators, ventilators, and backup generators, ensuring they are fully functional and accessible. For example, a hospital in a hurricane-prone area should test its emergency power systems monthly and stock sufficient fuel to sustain operations for at least 72 hours. Portable equipment, such as mobile X-ray units and point-of-care testing devices, should be pre-positioned in designated disaster response zones to enable rapid triage and treatment. Staff training on equipment use under stress conditions is equally critical, as even the most advanced tools are ineffective without skilled operators.
Facility preparedness completes the logistical triad, addressing the physical infrastructure that houses critical care operations. Hospitals must assess and reinforce structural vulnerabilities, such as securing windows in cyclone-prone regions or elevating electrical systems in flood-prone areas. Clear signage, unobstructed evacuation routes, and designated safe zones are essential for guiding patients and staff during emergencies. For instance, a hospital in an earthquake zone should install seismic locks on cabinets to prevent spills of hazardous materials and ensure that all heavy equipment is securely anchored. Regular drills simulating various disaster scenarios can identify bottlenecks in facility design and operational protocols, allowing for iterative improvements.
Integrating these logistical components requires a centralized command structure, often led by the hospital’s facilities management or emergency preparedness department. Collaboration with external stakeholders, such as local health departments, suppliers, and logistics providers, is vital for coordinating resource allocation and response efforts. For example, during wildfires, a hospital might partner with transportation companies to establish priority delivery routes for medical supplies. By adopting a holistic approach to logistics—one that prioritizes supply chain agility, equipment reliability, and facility resilience—hospitals can transform from passive responders to proactive guardians of community health in the face of disasters.
Monobeasts: The Two Point Hospital Challenge
You may want to see also
Frequently asked questions
The Emergency Management or Emergency Preparedness Department typically takes the lead in disaster preparedness within a hospital.
The Emergency Department is crucial in disaster preparedness as it serves as the first point of contact for victims and coordinates immediate response efforts.
The Infection Control Department ensures protocols are in place to prevent the spread of infectious diseases during a disaster, protecting both patients and staff.