Pacemakers, while life-saving devices that regulate irregular heart rhythms, can interfere with hospital heart monitors due to their electromagnetic signals. These signals, which control the heart’s pacing, often overlap with the frequencies used by ECG machines, leading to distorted readings or false alarms. Additionally, the electrical impulses from pacemakers can create artifacts on monitor displays, making it challenging for healthcare providers to accurately interpret a patient’s heart activity. This interference highlights the need for specialized monitoring techniques and equipment to ensure precise patient care in hospital settings.
| Characteristics | Values |
|---|---|
| Electromagnetic Interference (EMI) | Pacemakers emit low-level electromagnetic signals that can interfere with the sensitive electrodes and wiring of heart monitors, causing false readings or signal noise. |
| Artifact Generation | The electrical impulses from pacemakers can create artifacts on ECG traces, mimicking abnormal heart rhythms or obscuring true cardiac activity. |
| Frequency Overlap | Pacemakers operate at frequencies (typically 0.5–20 Hz) that overlap with the frequency range of heart monitor signals, leading to signal distortion or misinterpretation. |
| Sensing Issues | Heart monitors may incorrectly interpret pacemaker spikes as native cardiac signals, resulting in inaccurate heart rate or rhythm calculations. |
| Alarm Triggering | False alarms on heart monitors are common due to pacemaker interference, causing unnecessary clinical interventions or patient anxiety. |
| Device Compatibility | Not all heart monitors are designed to filter out pacemaker signals, exacerbating the issue in older or less advanced monitoring systems. |
| Patient Positioning | The proximity of the pacemaker to the heart monitor electrodes (e.g., in chest leads) increases the likelihood of interference. |
| Pacemaker Mode | Certain pacemaker modes (e.g., demand pacing) may produce more frequent or variable signals, increasing the risk of monitor interference. |
| Mitigation Strategies | Hospitals use specialized filters, alternative lead placements, or pacemaker programming adjustments to minimize interference. |
| Clinical Impact | While often manageable, pacemaker interference can delay accurate diagnosis or treatment, particularly in critical care settings. |
Explore related products






What You'll Learn
- Electromagnetic Interference: Pacemaker signals disrupt heart monitor readings due to overlapping frequencies
- Artifact Generation: Pacemaker impulses create false spikes on ECG tracings, mimicking arrhythmias
- Signal Overload: Combined pacemaker and heart signals overwhelm monitor processing capabilities
- Filtering Challenges: Monitors struggle to isolate heart signals from pacemaker electrical noise
- False Alarms: Pacemaker interference triggers unnecessary alerts, complicating patient monitoring accuracy
![]()
Electromagnetic Interference: Pacemaker signals disrupt heart monitor readings due to overlapping frequencies
Pacemakers and heart monitors are life-saving devices, but their interaction can lead to critical errors in patient monitoring. At the core of this issue is electromagnetic interference (EMI), where the frequencies emitted by pacemakers overlap with those used by heart monitors. This overlap causes signal distortion, making it difficult for monitors to accurately detect a patient’s natural heart rhythm. For instance, a pacemaker operating at frequencies between 30 and 50 Hz can interfere with the 0.5 to 40 Hz range typically monitored by ECG machines, leading to false arrhythmia alerts or missed cardiac events.
To mitigate this, healthcare providers must understand the frequency ranges of both devices. Pacemakers emit signals to regulate heartbeats, while heart monitors detect electrical activity within a specific bandwidth. When these ranges overlap, the monitor may misinterpret the pacemaker’s signal as the patient’s own heartbeat. For example, a dual-chamber pacemaker’s atrial pacing spike (around 35 Hz) can be misread as a premature atrial contraction, triggering unnecessary alarms. Hospitals should ensure monitors are calibrated to filter out pacemaker frequencies, though this requires specialized equipment and expertise.
Practical steps can reduce EMI-related disruptions. First, maintain a minimum distance of 15 cm between the pacemaker and the heart monitor’s electrodes, as proximity increases interference risk. Second, use EMI-shielded cables and devices, which are designed to block external signals. Third, regularly update both pacemakers and monitors to the latest firmware, as manufacturers often release patches to address interference issues. For patients over 65, who are more likely to have pacemakers, these precautions are especially critical due to their higher vulnerability to monitoring errors.
Despite these measures, complete elimination of EMI is challenging. Hospitals must adopt a layered approach, combining technical solutions with clinical vigilance. Staff should be trained to recognize pacemaker-related artifacts on monitor readings, such as pacing spikes or signal dropout. In cases of persistent interference, consider relocating the patient to a room with minimal electromagnetic activity or using alternative monitoring methods, like ultrasound, which is immune to EMI. By addressing the root cause—overlapping frequencies—hospitals can ensure accurate monitoring and better patient outcomes.
Ace Gangster Hospital Location: A Quick Guide to Finding Medical Help
You may want to see also
Explore related products





![]()
Artifact Generation: Pacemaker impulses create false spikes on ECG tracings, mimicking arrhythmias
Pacemakers, while life-saving devices, can confound hospital heart monitors by generating artifacts that mimic arrhythmias. These false spikes on ECG tracings arise from the electrical impulses emitted by the pacemaker, which the monitor interprets as abnormal heart activity. For instance, a pacemaker’s pacing spike, typically a sharp vertical deflection, can be mistaken for a premature ventricular contraction (PVC) if not recognized by the monitoring system or the clinician. This misinterpretation can lead to unnecessary alarms, diagnostic confusion, and even inappropriate interventions, such as administering antiarrhythmic medications or adjusting pacemaker settings.
To identify these artifacts, clinicians must understand their characteristic appearance. A pacing spike usually precedes the QRS complex and is distinct from the T wave or other native ECG features. For example, in a patient with a dual-chamber pacemaker, two spikes may appear—one atrial and one ventricular—depending on the pacing mode. Cross-referencing the ECG tracing with the pacemaker’s programmed settings (e.g., VVI, DDD) can confirm whether the spikes align with expected pacing behavior. In patients over 65, who constitute the majority of pacemaker recipients, this vigilance is critical due to the higher prevalence of comorbidities that could mask genuine arrhythmias.
A practical tip for distinguishing artifacts from true arrhythmias is to temporarily disable the pacemaker’s output (if clinically safe) or adjust the ECG filter settings. Most modern monitors allow for a "pacemaker filter" that reduces the amplitude of high-frequency artifacts, making the tracing easier to interpret. However, this filter should be used cautiously, as it may also obscure genuine high-frequency signals, such as those seen in atrial fibrillation. For patients on anticoagulants like warfarin (INR target 2.0–3.0) or direct oral anticoagulants, avoiding unnecessary interventions is particularly important to minimize bleeding risks.
Educating staff on pacemaker-ECG interactions is essential to prevent misinterpretation. For instance, a pacing spike in the T wave can mimic torsades de pointes if the clinician is unfamiliar with pacemaker artifacts. Simulation training with pacemaker patients’ ECGs can improve recognition accuracy. Additionally, integrating pacemaker data directly into the monitoring system, where available, can provide real-time correlation between pacing events and ECG changes. This dual-data approach reduces reliance on visual interpretation alone, enhancing diagnostic precision in high-stakes hospital settings.
Understanding the Role of a Hospital Scribe: Duties and Impact
You may want to see also
Explore related products






![]()
Signal Overload: Combined pacemaker and heart signals overwhelm monitor processing capabilities
Pacemakers emit distinct electrical signals to regulate heart rhythm, while heart monitors are designed to detect the heart’s natural electrical activity. When both signals coexist, their combined frequency and amplitude can exceed the processing thresholds of hospital monitors. For instance, a pacemaker’s spike, typically 0.5 to 5 volts, overlaps with the heart’s intrinsic 0.5 to 2 millivolt signal, creating a composite waveform that confuses algorithms. This overload manifests as artifactual arrhythmias, false alarms, or signal dropout, compromising patient monitoring accuracy.
Consider a scenario where a dual-chamber pacemaker operates at 70 beats per minute, synchronizing atrial and ventricular signals. The monitor, calibrated to isolate natural P and QRS complexes, struggles to differentiate between pacemaker spikes and organic electrical activity. This ambiguity triggers misinterpretation, such as flagging a stable rhythm as ventricular tachycardia. Clinicians must then manually verify readings, delaying critical interventions and increasing workload.
To mitigate signal overload, hospitals can employ adaptive filtering techniques. High-pass filters (cutoff >30 Hz) attenuate pacemaker spikes while preserving lower-frequency cardiac signals. Alternatively, software updates incorporating machine learning can train monitors to recognize and isolate pacemaker artifacts. Practical tips include adjusting lead placement to minimize spike amplitude and using dedicated pacemaker-compatible monitoring modes, if available.
Despite these solutions, challenges persist. Older monitors lack the computational power for real-time signal differentiation, necessitating hardware upgrades. Additionally, pacemaker variability—such as rate-responsive modes or MRI-compatible devices—introduces unpredictable signal patterns. Standardizing pacemaker-monitor interoperability and enhancing clinician training on artifact recognition are essential steps toward resolving this issue.
In summary, signal overload from combined pacemaker and heart signals is a technical bottleneck in hospital monitoring systems. Addressing it requires a multifaceted approach: algorithmic refinement, hardware upgrades, and clinical vigilance. By prioritizing these measures, healthcare providers can ensure accurate, uninterrupted patient monitoring in the presence of pacemakers.
Donate Masks: Help NYC Hospitals and Save Lives
You may want to see also
Explore related products






![]()
Filtering Challenges: Monitors struggle to isolate heart signals from pacemaker electrical noise
Pacemakers save lives by regulating heart rhythms, but their electrical signals can wreak havoc on hospital heart monitors. The core issue lies in the overlap of frequencies. Pacemakers emit pulses around 1-2 volts, typically at frequencies below 10 Hz, which unfortunately coincides with the range of a healthy heartbeat (0.5-3 Hz). This creates a filtering nightmare for monitors, which struggle to differentiate between the pacemaker's artificial signal and the patient's organic cardiac activity.
Example: Imagine trying to hear a whisper in a room where someone is constantly shouting. The whisper (heart signal) gets drowned out by the louder noise (pacemaker signal), making it difficult to discern the true rhythm.
This interference isn't just an annoyance; it has serious clinical implications. Misinterpretation of monitor readings can lead to incorrect diagnoses, inappropriate medication adjustments, or even unnecessary interventions. For instance, a pacemaker's signal might be misinterpreted as ventricular tachycardia, prompting unnecessary defibrillation. Conversely, a true arrhythmia could be masked by the pacemaker's signal, delaying critical treatment.
Analysis: The challenge lies in the limitations of current filtering algorithms. Traditional filters, designed for clean signals, are ill-equipped to handle the complex interplay between pacemaker and heart signals. More sophisticated techniques, like adaptive filtering and machine learning algorithms, show promise but require further development and validation before widespread clinical adoption.
Practical Tips for Healthcare Professionals:
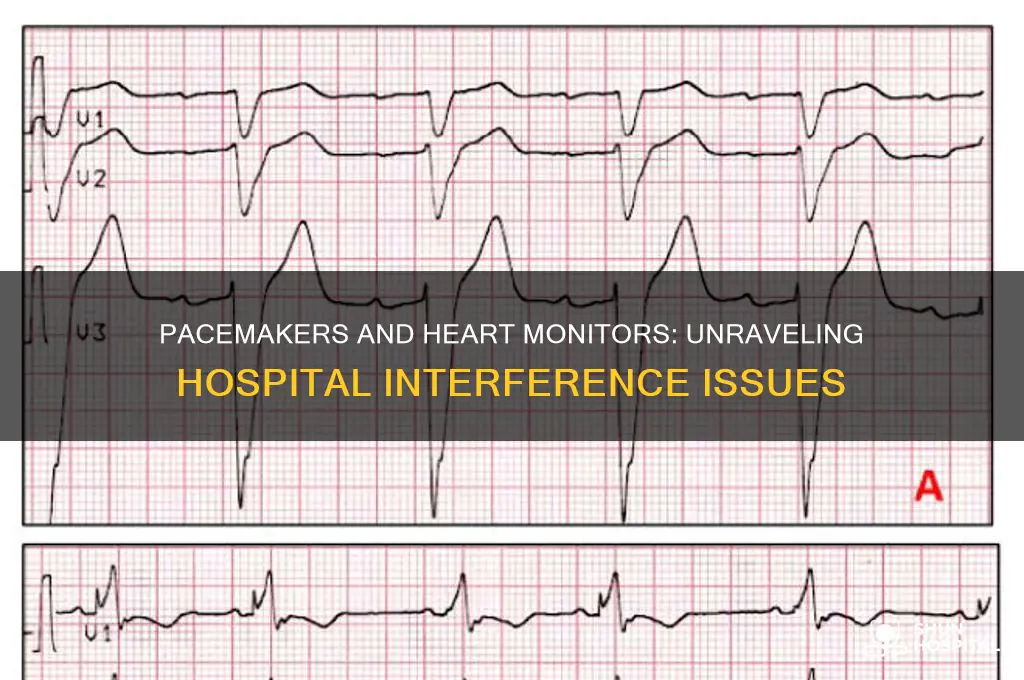
- Visual Inspection: Closely examine the monitor waveform for characteristic pacemaker spikes. These spikes are typically sharp and distinct from the undulating PQRST pattern of a normal heartbeat.
- Adjust Filter Settings: Experiment with different filter settings on the monitor. Some monitors allow for adjustable high-pass and low-pass filters, which can help attenuate the pacemaker signal while preserving the heart's rhythm.
- Alternative Monitoring Methods: Consider using alternative monitoring techniques like intracardiac electrograms (IEGMs) which directly record electrical activity within the heart, bypassing the interference from surface electrodes.
Takeaway: While pacemakers are life-saving devices, their interaction with heart monitors presents a significant filtering challenge. Understanding the underlying causes of this interference and employing appropriate strategies can help healthcare professionals accurately interpret monitor readings and ensure optimal patient care.
Saint Lukes Hospital Staff Scrubs: Styles, Colors, and Uniform Policies
You may want to see also
Explore related products






![]()
False Alarms: Pacemaker interference triggers unnecessary alerts, complicating patient monitoring accuracy
Pacemakers, while life-saving devices, can inadvertently disrupt hospital heart monitors, leading to false alarms that complicate patient care. This interference occurs because both pacemakers and heart monitors rely on electrical signals, and the pacemaker’s pulses can mimic or overlap with the heart’s natural rhythm, confusing the monitoring system. For instance, a pacemaker’s pacing spikes may be misinterpreted as premature ventricular contractions (PVCs), triggering alerts for arrhythmias that aren’t actually present. This phenomenon is particularly common in older pacemaker models or when the device’s settings are not optimized for the patient’s specific needs.
To mitigate this issue, healthcare providers must first identify the source of interference. A key step is to review the pacemaker’s programming and ensure it is synchronized with the patient’s heart rhythm. For example, adjusting the pacing mode from asynchronous (VOO) to demand-based modes (e.g., VVI or DDD) can reduce unnecessary signals. Additionally, using filtered monitoring settings on the heart monitor can help distinguish between pacemaker artifacts and true cardiac events. Nurses and technicians should be trained to recognize pacemaker spikes on ECG readings, which typically appear as small, vertical lines preceding the QRS complex.
Despite these measures, false alarms remain a persistent challenge, especially in high-acuity settings like intensive care units. A study published in the *Journal of Electrocardiology* found that up to 30% of alarms in pacemaker patients were false, leading to unnecessary interventions and increased stress for both patients and staff. This not only wastes valuable resources but can also desensitize healthcare providers to genuine alerts, potentially delaying critical care. Hospitals should implement protocols for verifying alarms in pacemaker patients, such as cross-referencing with physical assessments or using backup monitoring methods like pulse oximetry.
From a patient perspective, understanding this issue is crucial for reducing anxiety. If a pacemaker patient frequently experiences false alarms, they should communicate this to their healthcare team, who can then work with the electrophysiologist to fine-tune the device. Patients can also ask for a demonstration of how their pacemaker interacts with hospital monitors, empowering them to advocate for accurate monitoring. For older adults (ages 65+), who make up the majority of pacemaker recipients, family members or caregivers can play a vital role in ensuring consistent communication with medical staff.
In conclusion, while pacemaker interference with heart monitors is a complex issue, it is not insurmountable. By combining technical adjustments, staff education, and patient advocacy, hospitals can significantly reduce false alarms and improve monitoring accuracy. This not only enhances patient safety but also optimizes resource allocation, ensuring that healthcare providers can focus on genuine emergencies rather than being sidetracked by unnecessary alerts.
Partnering with Hospital Home Health Physical Therapy: A Comprehensive Guide
You may want to see also
Frequently asked questions
Pacemakers emit electrical signals to regulate heart rhythm, which can overlap with the signals heart monitors detect, causing interference or false readings.
While pacemakers can cause interference, they typically don’t completely stop heart monitors from working. However, they may require adjustments to the monitor settings for accurate readings.
Hospitals use specialized monitoring equipment and techniques, such as filtering out pacemaker signals or using alternative monitoring methods, to ensure accurate readings.
If not properly managed, pacemaker interference can lead to misinterpretation of heart rhythms, potentially affecting patient care. However, trained staff can minimize this risk.
No, the likelihood of interference depends on the pacemaker’s settings, the patient’s heart condition, and the type of heart monitor being used. Modern devices are designed to minimize interference.