Delayed cord clamping, the practice of waiting at least 30 to 60 seconds after birth before clamping and cutting the umbilical cord, is increasingly recommended by medical organizations due to its significant benefits for newborns. This approach allows for the transfer of additional blood volume from the placenta to the infant, which can improve iron stores, reduce anemia, and enhance neurodevelopmental outcomes. Despite these advantages, some hospitals may not consistently implement delayed cord clamping due to concerns about potential risks, such as jaundice or delayed resuscitation in high-risk births, or logistical challenges in busy delivery rooms. However, evidence suggests that the benefits far outweigh the risks for most infants, making it essential for healthcare providers to prioritize this practice and address barriers to its widespread adoption.
Explore related products






What You'll Learn
- Immediate Benefits for Baby: Delayed clamping improves iron stores, blood volume, and reduces anemia risk in newborns
- Stem Cell Transfer: Delayed clamping allows more stem cells to transfer from placenta to baby
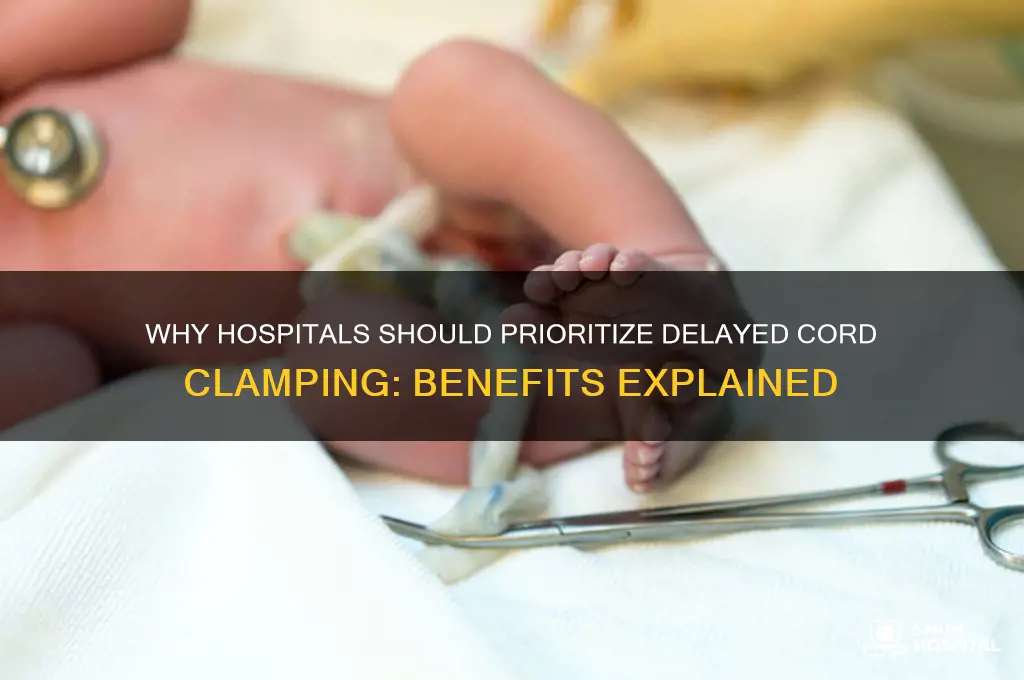
- Stability in Preterm Births: Preterm infants benefit from better blood pressure and reduced transfusion needs
- No Increased Jaundice Risk: Studies show delayed clamping does not significantly raise jaundice levels
- Maternal Benefits: Delayed clamping does not increase postpartum hemorrhage risk for mothers
![]()
Immediate Benefits for Baby: Delayed clamping improves iron stores, blood volume, and reduces anemia risk in newborns
Delayed cord clamping, the practice of waiting 30–60 seconds after birth before clamping and cutting the umbilical cord, offers significant immediate benefits for newborns, particularly in enhancing iron stores, optimizing blood volume, and reducing the risk of anemia. During the brief period after birth, a substantial volume of blood transfers from the placenta to the infant, providing a natural boost in blood volume. This additional blood contains vital components, including red blood cells rich in iron, which are essential for oxygen transport and overall health. For full-term infants, this process ensures they start life with a robust hematological foundation, reducing the likelihood of iron deficiency anemia in the first year.
One of the most critical immediate benefits of delayed cord clamping is the improvement in iron stores. Iron is crucial for brain development, immune function, and energy production. The placental blood transferred during delayed clamping can provide newborns with up to 50% more iron, which is particularly beneficial in settings where dietary iron intake may be insufficient. This natural iron supplementation can protect infants from anemia, a condition that can impair cognitive and motor development if left unaddressed. By simply delaying clamping, healthcare providers can ensure babies receive this essential nutrient without invasive interventions.
In addition to enhancing iron stores, delayed cord clamping significantly increases the newborn’s total blood volume. This additional blood volume supports cardiovascular stability, ensuring better perfusion of vital organs like the brain, heart, and kidneys. For preterm infants, this benefit is even more pronounced, as they are at higher risk of hypovolemia (low blood volume) due to their underdeveloped systems. By allowing the full transfer of placental blood, delayed clamping reduces the need for blood transfusions and other medical interventions, promoting a smoother transition to extrauterine life.
Another immediate advantage of delayed cord clamping is the reduced risk of anemia in newborns. Anemia in infancy can lead to fatigue, poor growth, and developmental delays. By maximizing iron stores and blood volume at birth, delayed clamping provides a protective effect against anemia, particularly in vulnerable populations such as preterm or low-birth-weight infants. This simple, cost-effective practice can have long-term implications for a child’s health and well-being, making it a critical consideration in neonatal care protocols.
Despite these clear benefits, some hospitals may still opt for immediate cord clamping due to misconceptions, time constraints, or outdated practices. However, the evidence supporting delayed clamping is compelling, and its implementation requires minimal changes to existing birthing procedures. By prioritizing delayed cord clamping, healthcare providers can ensure newborns receive the full physiological benefits of placental transfusion, setting them up for healthier outcomes from the very start of life. This practice aligns with the principle of doing no harm while actively promoting the immediate and long-term health of the infant.
The Role of a Ward Sister in Hospitals
You may want to see also
Explore related products





![]()
Stem Cell Transfer: Delayed clamping allows more stem cells to transfer from placenta to baby
Delayed cord clamping, the practice of waiting to clamp and cut the umbilical cord after birth, has gained significant attention for its potential benefits, one of which is enhanced stem cell transfer from the placenta to the newborn. During the moments immediately following birth, the umbilical cord continues to pulse, facilitating the transfer of blood rich in stem cells from the placenta to the baby. These stem cells, particularly hematopoietic stem cells, play a crucial role in the development of the baby’s immune system, blood, and other vital tissues. By delaying cord clamping, hospitals can ensure that a greater volume of this stem cell-rich blood is transferred, providing the newborn with a natural boost to their health and development.
Stem cells are unique in their ability to differentiate into various cell types, making them essential for tissue repair and immune system function. When cord clamping is delayed, typically for 1 to 3 minutes or until the cord stops pulsating, it allows for a more complete transfer of placental blood, which contains a higher concentration of stem cells compared to the baby’s blood at birth. This process not only increases the baby’s blood volume but also enhances their reserves of stem cells, which can be particularly beneficial for preterm infants or those at risk of conditions like anemia or immune disorders. Despite these advantages, many hospitals still opt for immediate cord clamping due to long-standing practices, lack of awareness, or concerns about potential risks, which are often unfounded.
The mechanism behind stem cell transfer during delayed cord clamping is straightforward yet profound. As the placenta continues to contract after birth, it actively pumps blood through the umbilical cord to the baby. This blood is rich in stem cells, iron, and other essential nutrients that support the baby’s growth and development. Immediate cord clamping interrupts this natural process, leaving a significant portion of the placental blood—and its stem cells—in the placenta, which is typically discarded. By allowing this transfer to complete, delayed clamping ensures the baby receives a full complement of stem cells, which can improve long-term health outcomes and reduce the need for interventions like blood transfusions.
Research supports the idea that delayed cord clamping maximizes stem cell transfer, with studies showing higher levels of hematopoietic stem cells in infants who undergo this practice. These stem cells contribute to the formation of red and white blood cells, platelets, and other immune components, reducing the risk of infections and blood disorders in early childhood. Additionally, the iron supplied through delayed clamping helps prevent anemia, a common issue in infants, particularly those born prematurely. Despite these proven benefits, the adoption of delayed cord clamping remains inconsistent across hospitals, often due to outdated protocols or a lack of training among medical staff.
In conclusion, delayed cord clamping is a simple yet powerful intervention that significantly enhances stem cell transfer from the placenta to the baby. By allowing the natural process of placental transfusion to complete, hospitals can provide newborns with a rich supply of stem cells, iron, and other vital components that support their immediate and long-term health. The evidence supporting this practice is robust, and its implementation should be prioritized to ensure that every baby receives the full benefits of this natural process. Hospitals that continue to practice immediate cord clamping without medical necessity are missing a critical opportunity to improve neonatal outcomes and set the stage for healthier childhood development.
Visiting Hours: Should Family Be Exempt?
You may want to see also
Explore related products






![]()
Stability in Preterm Births: Preterm infants benefit from better blood pressure and reduced transfusion needs
Delayed cord clamping (DCC) has emerged as a critical practice in neonatal care, particularly for preterm infants, due to its profound impact on stability, blood pressure regulation, and reduced transfusion requirements. Preterm infants often face challenges related to immature cardiovascular systems, making them susceptible to hypotension and anemia. DCC allows for the physiological transfer of placental blood to the infant, which typically provides 20-30% of the total blood volume. This additional volume is rich in red blood cells, stem cells, and volume-expanding fluids, which help stabilize the infant’s circulation immediately after birth. By ensuring a smoother transition from fetal to neonatal life, DCC reduces the risk of hypotension, a common issue in preterm infants that can lead to organ underperfusion and long-term complications.
One of the most significant benefits of DCC in preterm births is the improvement in blood pressure stability. Placental transfusion increases preload to the heart, enhancing cardiac output and systemic blood flow. This is particularly crucial for preterm infants, whose underdeveloped cardiovascular systems struggle to compensate for rapid changes in circulation. Studies have shown that preterm infants who undergo DCC have higher mean blood pressure in the first hours of life compared to those with immediate cord clamping. This stability reduces the need for inotropic support and minimizes the risk of necrotizing enterocolitis (NEC) and intraventricular hemorrhage (IVH), conditions often exacerbated by poor perfusion.
Another critical advantage of DCC in preterm infants is the reduction in transfusion needs. Preterm infants are at high risk of anemia due to their limited erythropoietic capacity and frequent blood draws for laboratory tests. By receiving a larger volume of placental blood, these infants start life with higher hemoglobin levels, delaying the onset of anemia and reducing the frequency of red blood cell transfusions. This not only conserves blood products but also lowers the risk of transfusion-related complications, such as infection or alloimmunization. The iron reserves from placental blood also support brain development and reduce the need for iron supplementation in the early weeks of life.
Furthermore, DCC contributes to overall hemodynamic stability in preterm infants by optimizing volume status and reducing the need for fluid resuscitation. Immediate cord clamping can lead to a sudden reduction in venous return, causing transient hypotension and tachycardia. In contrast, DCC allows for a gradual adjustment of the infant’s circulation, minimizing stress on the heart and lungs. This is especially beneficial for extremely preterm infants, who are more vulnerable to cardiovascular instability. By promoting better volume status, DCC also supports renal perfusion, reducing the risk of acute kidney injury and improving urine output in the critical early hours.
In conclusion, delayed cord clamping plays a pivotal role in achieving stability in preterm births by improving blood pressure regulation and reducing transfusion needs. The physiological benefits of placental transfusion, including enhanced cardiac output, higher hemoglobin levels, and better volume status, address the unique vulnerabilities of preterm infants. As evidence continues to support the advantages of DCC, its adoption in neonatal care is essential to optimize outcomes for these fragile infants. Hospitals that prioritize this practice contribute significantly to reducing morbidity and mortality in preterm populations.
Ukraine Maternity Hospital: Empty or Full of Lies?
You may want to see also
Explore related products




![]()
No Increased Jaundice Risk: Studies show delayed clamping does not significantly raise jaundice levels
One of the primary concerns surrounding delayed cord clamping (DCC) has been the potential for increased neonatal jaundice, a condition caused by elevated bilirubin levels in the blood. However, numerous studies have addressed this concern, consistently demonstrating that delayed cord clamping does not significantly raise the risk of jaundice. A 2017 meta-analysis published in *The Lancet* reviewed data from over 3,000 infants and found no clinically significant difference in jaundice rates between delayed and immediate cord clamping groups. This finding is crucial, as it reassures healthcare providers and parents that DCC can be safely implemented without exacerbating jaundice-related complications.
Further research has reinforced these conclusions. A study published in *Pediatrics* in 2019 specifically examined bilirubin levels in newborns following delayed cord clamping and found no statistically significant increase in hyperbilirubinemia compared to immediate clamping. The study also noted that any slight elevation in bilirubin levels observed in the DCC group was transient and did not require additional medical intervention. These results align with guidelines from the World Health Organization (WHO) and the American College of Obstetricians and Gynecologists (ACOG), which both advocate for delayed cord clamping due to its benefits, including improved iron stores and circulatory stability, without an increased risk of jaundice.
Clinically, the fear of jaundice should not deter hospitals from adopting delayed cord clamping practices. While it is true that bilirubin levels may temporarily rise due to the additional transfusion of placental blood, this increase is generally mild and manageable. Standard monitoring protocols for jaundice, such as bilirubin level checks and clinical assessments, remain effective regardless of cord clamping timing. Moreover, the long-term benefits of DCC, such as reduced anemia and improved neurodevelopmental outcomes, far outweigh the minimal and transient risk of jaundice.
Educating healthcare providers and parents about these findings is essential to dispel misconceptions and promote the adoption of delayed cord clamping. Hospitals can play a pivotal role by updating their protocols to reflect evidence-based practices and ensuring staff are trained to monitor newborns appropriately. By doing so, institutions can maximize the benefits of DCC while minimizing unwarranted concerns about jaundice. The evidence is clear: delayed cord clamping does not significantly increase the risk of jaundice, making it a safe and beneficial practice for newborns.
In conclusion, the body of research on delayed cord clamping and jaundice risk is robust and reassuring. Studies consistently show that DCC does not lead to clinically significant increases in jaundice levels, and any minor elevations in bilirubin are transient and manageable. Hospitals should feel confident in implementing delayed cord clamping as a standard practice, knowing that it provides substantial benefits to newborns without raising the risk of jaundice-related complications. This evidence-based approach aligns with global health recommendations and represents best practices in neonatal care.
Denver, Colorado's Hospital Network: A Comprehensive Overview
You may want to see also
Explore related products


$9.99




![]()
Maternal Benefits: Delayed clamping does not increase postpartum hemorrhage risk for mothers
Delayed cord clamping (DCC), the practice of waiting at least 30–60 seconds after birth before clamping and cutting the umbilical cord, has been widely studied for its benefits to newborns, including improved iron stores and developmental outcomes. However, concerns about its impact on maternal health, particularly the risk of postpartum hemorrhage (PPH), have persisted. Evidence from numerous randomized controlled trials and systematic reviews consistently demonstrates that delayed cord clamping does not increase the risk of PPH in mothers. This reassurance is crucial for healthcare providers and parents, as it removes a significant barrier to implementing DCC as a standard practice.
One of the primary reasons delayed cord clamping does not elevate PPH risk is the physiological process of placental transfusion. During DCC, blood from the placenta continues to flow to the infant, but this process is gradual and does not interfere with the natural detachment of the placenta or the uterus’s ability to contract and control bleeding. Studies, such as those published in the *New England Journal of Medicine* and *The Lancet*, have shown no significant difference in PPH rates between women who underwent immediate cord clamping and those who had delayed clamping. This finding holds true across various populations, including women at higher risk for bleeding, such as those with anemia or previous PPH.
Another factor contributing to the safety of DCC for mothers is the timing of uterotonic administration. Uterotonics, such as oxytocin, are commonly used to prevent PPH by promoting uterine contraction. Research indicates that administering these medications immediately after birth, rather than waiting for cord clamping, effectively mitigates bleeding risks. This practice ensures that maternal safety is prioritized while still allowing for the benefits of delayed clamping. The World Health Organization (WHO) and other leading health bodies now recommend this approach as part of their guidelines for DCC.
Furthermore, the volume of blood transferred during delayed cord clamping is relatively small and does not deplete maternal blood volume to a degree that increases hemorrhage risk. On average, DCC results in an additional 20–30 mL of blood loss for the mother, which is clinically insignificant compared to the total blood volume. This minimal loss is far outweighed by the benefits to the newborn, making DCC a safe and advantageous practice for both mother and baby.
In conclusion, the evidence overwhelmingly supports the safety of delayed cord clamping for mothers, particularly regarding postpartum hemorrhage risk. Healthcare providers can confidently adopt DCC as a standard of care, knowing it does not compromise maternal health. By addressing misconceptions and emphasizing the physiological mechanisms at play, hospitals can promote this practice more widely, ensuring optimal outcomes for both newborns and their mothers.
Absorbent Cotton Wool: Hospital-Grade Essentials
You may want to see also
Frequently asked questions
Hospitals often delay cord clamping and cutting to allow more blood from the placenta to transfer to the newborn, which can improve iron stores, blood volume, and overall health in the infant.
Delaying cord clamping and cutting can increase hemoglobin levels, reduce anemia, and improve developmental outcomes in newborns, especially in preterm infants.
While rare, delaying cord clamping may slightly increase the risk of jaundice in newborns, though this is typically manageable with proper monitoring and treatment.
The World Health Organization (WHO) recommends delaying cord clamping for at least 1 to 3 minutes after birth for all infants, or until the cord stops pulsating, to maximize benefits.