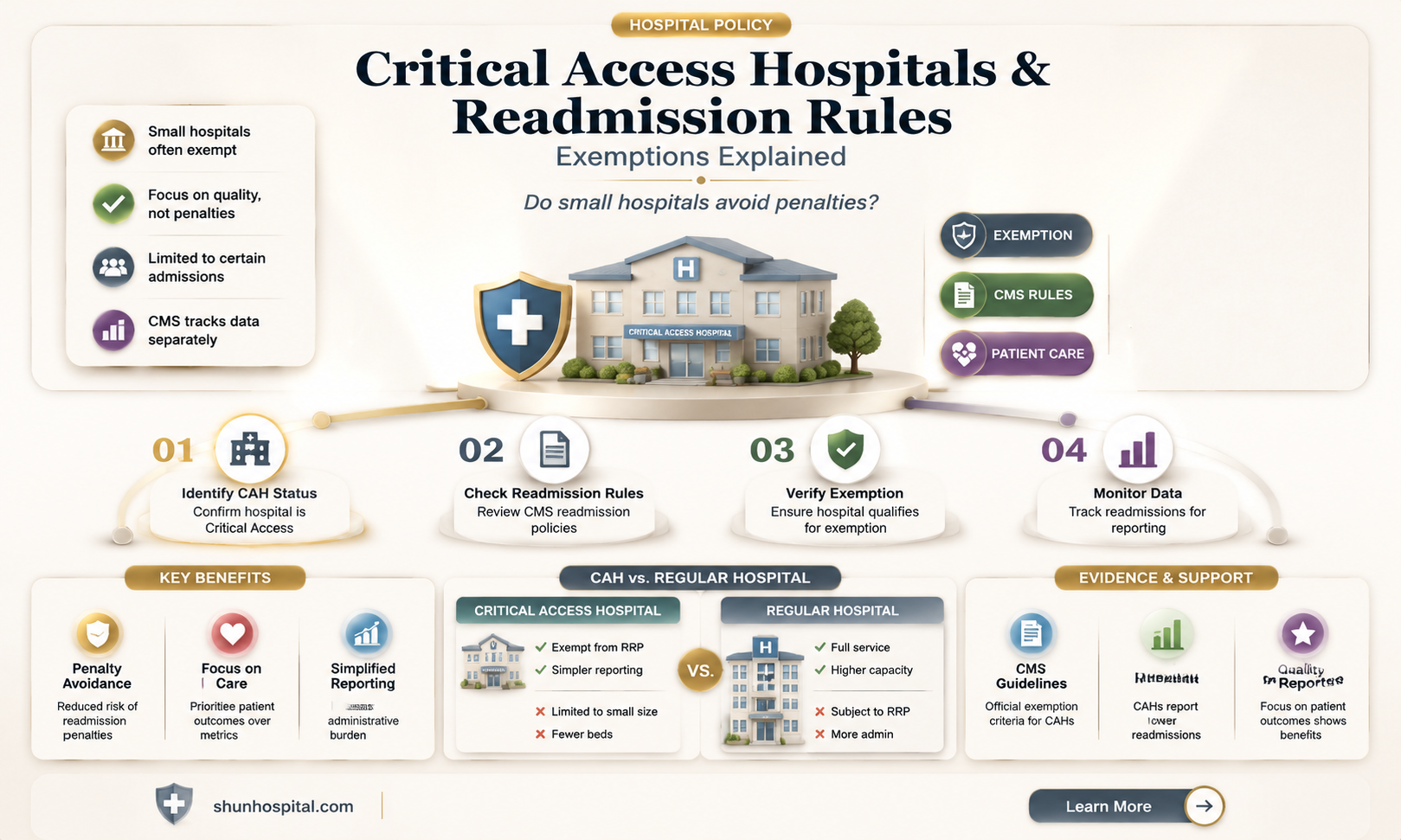
Critical Access Hospitals (CAHs), which are small, rural facilities designated to ensure healthcare access in underserved areas, have long been subject to unique regulatory considerations due to their limited resources and patient populations. One key question that arises is whether CAHs are exempt from the Hospital Readmissions Reduction Program (HRRP), a Medicare initiative aimed at reducing preventable readmissions by penalizing hospitals with higher-than-expected readmission rates. While CAHs are not entirely exempt from the HRRP, they do receive certain accommodations, such as exclusion from penalties for specific conditions like chronic obstructive pulmonary disease (COPD) and pneumonia, and they are evaluated based on a smaller subset of conditions compared to larger hospitals. These adjustments reflect the recognition of the challenges CAHs face in managing readmissions, balancing accountability with the realities of rural healthcare delivery.
| Characteristics | Values |
|---|---|
| Exemption Status | Critical Access Hospitals (CAHs) are exempt from the Hospital Readmissions Reduction Program (HRRP). |
| Reason for Exemption | CAHs are excluded due to their small size, limited resources, and unique patient populations, which make it challenging to apply the same readmission penalties as larger hospitals. |
| Program Applicability | The HRRP applies to acute care hospitals, including prospective payment system (PPS) hospitals, but explicitly excludes CAHs. |
| CMS Policy | The Centers for Medicare & Medicaid Services (CMS) has not included CAHs in the HRRP since its inception in 2012. |
| Readmission Penalties | CAHs do not face financial penalties for excess readmissions under the HRRP. |
| Reporting Requirements | While exempt from penalties, CAHs may still be required to report readmission data for quality improvement purposes. |
| Alternative Quality Programs | CAHs participate in other CMS quality programs, such as the Medicare Beneficiary Quality Improvement Program (MBQIP), which focuses on rural hospital performance. |
| Legislative Basis | The exemption is based on the Social Security Act and subsequent CMS regulations that differentiate CAHs from other hospital types. |
| Patient Population Impact | The exemption acknowledges the unique challenges CAHs face in managing readmissions due to serving rural, often underserved populations. |
| Recent Updates (as of latest data) | No recent changes have been made to include CAHs in the HRRP, maintaining their exempt status. |
Explore related products






What You'll Learn
![]()
Definition of Critical Access Hospitals
Critical Access Hospitals (CAHs) are a vital component of the U.S. healthcare system, particularly in rural areas where access to medical services is limited. Established by the Balanced Budget Act of 1997, CAHs are designed to ensure that residents of rural communities have reasonable access to essential healthcare services. To qualify as a CAH, a facility must meet specific criteria set by the Centers for Medicare & Medicaid Services (CMS). These criteria include being located in a rural area, maintaining no more than 25 acute care inpatient beds, and providing 24/7 emergency care services. Additionally, CAHs must be certified by their state and meet all applicable federal requirements for participation in Medicare.
One of the defining features of CAHs is their focus on serving rural populations, which often face unique healthcare challenges due to geographic isolation, lower population density, and limited resources. CAHs are intended to provide essential services such as inpatient care, outpatient care, and emergency medical services, ensuring that rural residents do not have to travel long distances for basic healthcare needs. The designation also allows CAHs to receive cost-based reimbursement from Medicare, which helps sustain their operations in areas where patient volumes are typically lower compared to urban hospitals.
The designation of a hospital as a CAH comes with specific operational and regulatory requirements. For instance, CAHs must have an annual average length of stay of 96 hours or less for acute care patients and must be located more than 35 miles from another hospital, or 15 miles in areas with mountainous terrain or only secondary roads. These requirements ensure that CAHs are strategically positioned to serve their communities effectively. Furthermore, CAHs are subject to less stringent regulatory standards compared to larger hospitals, which helps reduce administrative burdens and operational costs.
In the context of the Readmission Reduction Program, understanding the definition of CAHs is crucial. The Readmission Reduction Program, established by the Affordable Care Act, aims to reduce hospital readmissions by penalizing hospitals with higher-than-expected readmission rates for certain conditions. However, CAHs are generally exempt from this program due to their unique role in rural healthcare and the challenges they face in managing patient populations. This exemption recognizes the distinct operational and financial constraints of CAHs and ensures that they are not unfairly penalized for factors beyond their control.
In summary, Critical Access Hospitals are specialized healthcare facilities designed to provide essential services to rural communities. Their designation is based on specific criteria related to size, location, and services offered, and they play a critical role in ensuring healthcare access for underserved populations. The exemption of CAHs from the Readmission Reduction Program highlights the recognition of their unique challenges and the importance of supporting their continued operation in rural areas. By understanding the definition and purpose of CAHs, policymakers and healthcare providers can better address the needs of rural populations and ensure equitable access to care.
When Should Hospitals Query the NPDB: Key Compliance Insights
You may want to see also
Explore related products






![]()
Readmission Reduction Program Overview
The Readmission Reduction Program (RRP) is a Medicare initiative aimed at improving the quality of care and reducing avoidable hospital readmissions. Established by the Affordable Care Act (ACA) in 2010, the program financially incentivizes hospitals to enhance patient care transitions and follow-up, thereby decreasing the likelihood of patients returning to the hospital within 30 days of discharge. Hospitals with higher-than-expected readmission rates for specific conditions—such as heart attacks, heart failure, pneumonia, chronic obstructive pulmonary disease (COPD), and total hip/knee replacements—face financial penalties in the form of reduced Medicare reimbursements. The program’s primary goal is to encourage hospitals to implement evidence-based practices that improve patient outcomes and reduce healthcare costs associated with preventable readmissions.
Critical Access Hospitals (CAHs), which are small, rural facilities designated to provide essential healthcare services to underserved communities, have a unique position within the RRP. As of current regulations, CAHs are exempt from the Readmission Reduction Program. This exemption is rooted in the recognition of the distinct challenges faced by rural hospitals, including limited resources, smaller patient volumes, and higher proportions of patients with complex, chronic conditions. These factors can make it difficult for CAHs to achieve readmission rates comparable to those of larger, urban hospitals. The exemption ensures that CAHs are not unfairly penalized for circumstances beyond their control, allowing them to focus on maintaining access to care in rural areas without the added financial burden of RRP penalties.
Despite their exemption, CAHs are still encouraged to adopt strategies to reduce readmissions and improve patient care. Many CAHs voluntarily implement care coordination programs, patient education initiatives, and post-discharge follow-up protocols to enhance outcomes. While not subject to RRP penalties, these efforts align with broader healthcare quality goals and can lead to better patient satisfaction and reduced healthcare utilization. Additionally, CAHs may participate in other Medicare quality improvement programs, such as the Hospital Value-Based Purchasing Program, which rewards hospitals for meeting certain performance standards.
The exemption of CAHs from the RRP highlights the importance of tailoring healthcare policies to the specific needs of different hospital types. Rural hospitals play a critical role in providing access to care for vulnerable populations, and their exclusion from the program acknowledges the unique operational and financial constraints they face. However, this exemption does not diminish the importance of addressing readmissions in rural settings. Policymakers and healthcare leaders continue to explore alternative approaches to support CAHs in reducing readmissions, such as providing technical assistance, funding for care coordination initiatives, and data-sharing tools to identify areas for improvement.
In summary, the Readmission Reduction Program is a key component of Medicare’s efforts to enhance healthcare quality and efficiency by reducing preventable hospital readmissions. While Critical Access Hospitals are exempt from the program due to their unique challenges, they remain integral to the broader goal of improving patient outcomes. The exemption ensures that CAHs can continue serving rural communities without facing undue financial penalties, while still encouraging them to adopt best practices for reducing readmissions. This targeted approach reflects a balanced effort to address healthcare disparities and promote equitable access to high-quality care across all hospital settings.
Border Crosser Concerns: Harris County Hospital District Policies Explained
You may want to see also
Explore related products



$9.99 $14.99



![]()
Exemption Criteria for CAHs
Critical Access Hospitals (CAHs) play a vital role in providing healthcare services to rural and underserved communities. However, their unique operational and financial challenges have prompted specific considerations regarding their participation in various federal programs, including the Hospital Readmissions Reduction Program (HRRP). The HRRP, established by the Affordable Care Act, aims to reduce avoidable readmissions by penalizing hospitals with higher-than-expected readmission rates. For CAHs, understanding the exemption criteria from this program is crucial for financial stability and operational planning.
One of the primary exemption criteria for CAHs is their designation under the Medicare Rural Hospital Flexibility (Flex) Program. CAHs are automatically exempt from the HRRP if they are part of this program, which is designed to support small rural hospitals in improving their quality of care and financial performance. This exemption recognizes the inherent challenges CAHs face, such as limited resources, smaller patient volumes, and higher proportions of Medicare beneficiaries, which can skew readmission rate calculations.
Another exemption criterion is based on patient volume. CAHs with fewer than 100 Medicare discharges in the measurement period are exempt from the HRRP. This threshold acknowledges that hospitals with low patient volumes may not have statistically significant data to accurately measure readmission rates. Additionally, the small sample size could lead to volatile and unreliable performance metrics, making it unfair to penalize these hospitals based on limited data.
Geographic and demographic factors also play a role in exemption criteria. CAHs located in rural areas with limited access to healthcare services are often exempt, as are those serving a high percentage of low-income or medically underserved populations. These exemptions reflect the understanding that such hospitals face unique challenges in managing patient care and reducing readmissions, often due to factors beyond their control, such as patient transportation barriers or lack of access to follow-up care.
Lastly, CAHs may be exempt if they participate in certain quality improvement initiatives or demonstrate significant efforts to reduce readmissions despite their resource constraints. For example, involvement in programs like the Medicare Beneficiary Quality Improvement Project (MBQIP) can qualify a CAH for exemption. This criterion encourages CAHs to actively engage in quality improvement activities while recognizing their limitations compared to larger, urban hospitals.
In summary, the exemption criteria for CAHs from the HRRP are multifaceted, taking into account their designation under the Flex Program, patient volume, geographic location, demographic challenges, and participation in quality improvement initiatives. These criteria aim to balance the goals of reducing avoidable readmissions with the realities of operating a small, rural hospital. By understanding and leveraging these exemptions, CAHs can focus on delivering essential healthcare services to their communities without undue financial strain.
Palm Beach County: Hospitals and Healthcare Availability
You may want to see also
Explore related products






![]()
Impact on CAH Funding
Critical Access Hospitals (CAHs) play a vital role in providing healthcare services to rural communities across the United States. However, their financial stability is often precarious due to limited patient volumes, higher operating costs, and reliance on federal reimbursement programs. The question of whether CAHs are exempt from the Hospital Readmissions Reduction Program (HRRP) is significant because it directly impacts their funding. The HRRP, established under the Affordable Care Act, penalizes hospitals with higher-than-expected readmission rates by reducing their Medicare reimbursements. If CAHs are not exempt, they face financial penalties that could exacerbate their already strained budgets.
The impact on CAH funding is twofold. First, CAHs typically serve a patient population with higher rates of chronic conditions, socioeconomic challenges, and limited access to follow-up care, all of which increase the likelihood of readmissions. If CAHs are subject to HRRP penalties, they may lose a substantial portion of their Medicare reimbursements, which account for a significant share of their revenue. This reduction in funding could force CAHs to cut essential services, delay investments in infrastructure, or even risk closure, leaving rural communities without access to critical healthcare services.
Second, the administrative burden of complying with HRRP requirements adds another layer of financial strain. CAHs often operate with limited staff and resources, making it challenging to implement robust care coordination and transitional care programs necessary to reduce readmissions. Diverting resources to meet HRRP standards could detract from other critical areas, such as patient care and community outreach, further compromising their ability to serve their populations effectively.
However, if CAHs are exempt from the HRRP, they can avoid these financial penalties and allocate their resources more strategically. Exemption would provide CAHs with greater financial stability, enabling them to focus on improving patient outcomes without the looming threat of reduced reimbursements. It would also allow them to invest in programs tailored to their unique patient populations, such as telemedicine, home health services, and chronic disease management, which could indirectly reduce readmissions over time.
In conclusion, the exemption status of CAHs from the HRRP has a profound impact on their funding and, by extension, their ability to serve rural communities. Subjecting CAHs to HRRP penalties risks destabilizing their finances and compromising access to care, while exemption would provide much-needed relief and flexibility. Policymakers must carefully consider the unique challenges faced by CAHs when designing and implementing programs like the HRRP to ensure that rural healthcare remains viable and sustainable.
When Do Hospitals Schedule Life Support Discontinuation: Ethical Insights
You may want to see also
Explore related products




![]()
Compliance and Reporting Requirements
Critical Access Hospitals (CAHs) face unique compliance and reporting requirements when it comes to the Hospital Readmissions Reduction Program (HRRP), a Centers for Medicare & Medicaid Services (CMS) initiative aimed at reducing avoidable readmissions. While CAHs are generally subject to less stringent regulations compared to larger hospitals, they are not entirely exempt from HRRP. Understanding the specific compliance and reporting obligations is crucial for CAHs to avoid penalties and maintain their Medicare participation.
Under the HRRP, CAHs are required to report readmission data for specific conditions, including acute myocardial infarction (AMI), heart failure (HF), chronic obstructive pulmonary disease (COPD), and pneumonia. This data is collected through Medicare claims and is used to calculate readmission rates. CAHs must ensure accurate and timely submission of claims data to CMS, as this forms the basis for their readmission metrics. Failure to comply with reporting requirements can result in data suppression, which may lead to penalties or exclusion from HRRP calculations.
Compliance also involves adhering to CMS guidelines for data validation and quality assurance. CAHs must verify the accuracy of their submitted claims data and address any discrepancies promptly. Additionally, CAHs should implement internal processes to monitor readmission rates and identify areas for improvement. This includes tracking patient outcomes, analyzing readmission trends, and developing strategies to reduce preventable readmissions. CMS provides resources and tools to assist CAHs in this process, such as the Quality Net portal, which offers access to performance feedback reports.
Reporting requirements extend beyond data submission to include participation in quality improvement initiatives. CAHs are encouraged to engage in programs like the Hospital Improvement Innovation Network (HIIN) to enhance their readmission reduction efforts. These initiatives often provide technical assistance, best practices, and benchmarking opportunities to help CAHs meet HRRP goals. By actively participating in such programs, CAHs can demonstrate their commitment to compliance and continuous quality improvement.
Finally, CAHs must stay informed about updates to HRRP policies and reporting standards. CMS periodically revises the program’s methodology, condition-specific measures, and penalty structures. CAHs should regularly review CMS communications, attend webinars, and consult with healthcare associations to ensure they remain compliant with the latest requirements. Proactive engagement with these changes will help CAHs avoid penalties and maintain their eligibility for Medicare reimbursement.
In summary, while CAHs are not exempt from the HRRP, their compliance and reporting requirements are tailored to their unique operational and resource constraints. Accurate data reporting, adherence to CMS guidelines, participation in quality improvement initiatives, and staying informed about program updates are essential for CAHs to navigate the HRRP successfully. By prioritizing these obligations, CAHs can minimize financial risks and contribute to improved patient outcomes.
Exploring Lafayette's Hospital Drive: Boulevard or Not?
You may want to see also
Frequently asked questions
Yes, Critical Access Hospitals are exempt from the HRRP, as confirmed by the Centers for Medicare & Medicaid Services (CMS).
CAHs are exempt because they typically serve rural areas with lower patient volumes, making it challenging to accurately measure readmission rates and ensure fair comparisons with larger hospitals.
No, CAHs do not face penalties under the HRRP, but they are still encouraged to focus on improving care quality and reducing avoidable readmissions.
While CAHs are exempt from HRRP penalties, they may still be required to report readmission data for quality improvement and monitoring purposes, depending on CMS guidelines.
No, CAHs cannot voluntarily participate in the HRRP, as the program specifically excludes them due to their unique operational and patient population characteristics.