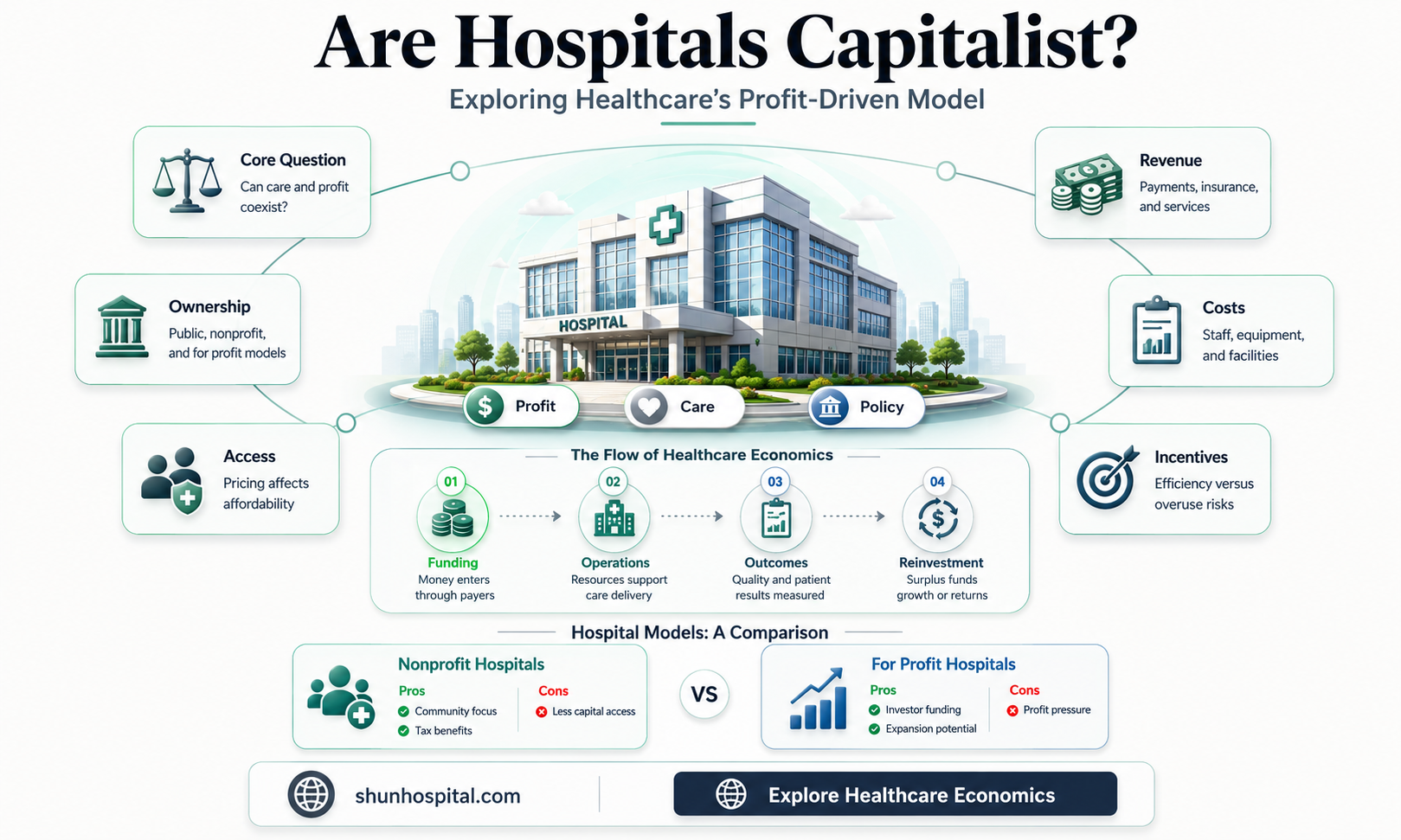
The question of whether hospitals are capitalist institutions sparks a complex debate at the intersection of healthcare, economics, and ethics. While hospitals are primarily dedicated to providing medical care, their operation within a market-driven system often aligns them with capitalist principles. Many hospitals, especially in countries like the United States, function as profit-driven entities, charging fees for services, relying on insurance payments, and sometimes prioritizing financial sustainability over universal access to care. This model raises concerns about inequities in healthcare access, as those without sufficient resources may face barriers to treatment. Conversely, proponents argue that capitalism fosters innovation and efficiency in healthcare delivery. Ultimately, the capitalist nature of hospitals depends on their funding structures, ownership models, and the balance between profit motives and the ethical imperative to serve all patients equitably.
Explore related products






What You'll Learn
- Profit-driven healthcare: Prioritizing financial gain over patient care in hospital management and decision-making
- Privatization of services: Shifting public healthcare to private, for-profit models and its societal impact
- Cost of treatment: High medical expenses and their effect on accessibility and patient outcomes
- Pharmaceutical influence: Drug companies' role in hospital operations and treatment protocols for profit
- Labor exploitation: Underpaid healthcare workers and its connection to capitalist hospital systems
![]()
Profit-driven healthcare: Prioritizing financial gain over patient care in hospital management and decision-making
Hospitals, once primarily seen as sanctuaries of healing, increasingly operate under a profit-driven model that prioritizes financial gain over patient care. This shift is evident in the rise of for-profit hospitals, which now account for approximately 20% of all U.S. hospitals. Unlike their nonprofit counterparts, these institutions are beholden to shareholders, driving decisions that maximize revenue rather than optimize patient outcomes. For instance, for-profit hospitals are more likely to perform lucrative elective procedures, such as joint replacements or cardiac surgeries, while underinvesting in less profitable services like mental health or emergency care. This misalignment of incentives raises ethical questions: should healthcare be a commodity, or a fundamental human right?
Consider the practice of "upcoding," where hospitals inflate the severity of a patient's condition to bill insurers for higher reimbursements. A 2020 study found that upcoding costs Medicare billions annually, diverting funds from actual patient needs. Similarly, the push to shorten hospital stays, often driven by cost-cutting measures, can lead to premature discharges. Patients, particularly the elderly or those with chronic conditions, may end up readmitted within weeks, exacerbating their health issues and increasing overall healthcare costs. These practices illustrate how financial motives can undermine the quality and continuity of care.
To mitigate the impact of profit-driven healthcare, patients must become proactive advocates for their own care. Start by questioning the necessity of recommended procedures or tests, especially if they seem unrelated to your primary condition. Request itemized bills to identify and dispute potential upcoding or unnecessary charges. For example, a routine blood test should cost around $10–$20, not $200. Additionally, consider seeking care at nonprofit or community health centers, which are more likely to prioritize patient needs over profit margins. Tools like the Hospital Compare website can help evaluate hospitals based on quality metrics rather than financial performance.
A comparative analysis of healthcare systems highlights the consequences of prioritizing profit. In countries with universal healthcare, such as Canada or the UK, hospitals operate under budgets that emphasize accessibility and preventive care. In contrast, the U.S. system, where private insurance and out-of-pocket costs dominate, incentivizes high-cost interventions. For instance, the U.S. spends nearly twice as much per capita on healthcare as Canada but has lower life expectancy and higher infant mortality rates. This disparity underscores the need for systemic reforms that decouple healthcare from profit motives, ensuring that patient care remains the ultimate priority.
Luke Perry Hospitalized: 90210 Star Suffers Stroke, Fans Concerned
You may want to see also
Explore related products


$0.99 $29.99



![]()
Privatization of services: Shifting public healthcare to private, for-profit models and its societal impact
The privatization of healthcare services, a growing global trend, raises critical questions about accessibility, quality, and equity. As public healthcare systems face budgetary constraints and increasing demands, governments are turning to private, for-profit models to bridge the gap. This shift, however, is not without consequences. Consider the United Kingdom’s National Health Service (NHS), where private providers now handle a significant portion of non-emergency surgeries, diagnostics, and even primary care. While this has reduced wait times for some, it has also created a two-tier system where those who can afford private care receive faster, often better treatment, while the less affluent rely on an overburdened public system. This disparity underscores a fundamental tension: privatization can improve efficiency and innovation but often at the expense of universal access.
To understand the societal impact, examine the case of Chile, where healthcare is largely privatized. Here, private insurance plans offer shorter wait times and access to advanced treatments, but they come with high premiums that exclude lower-income individuals. As a result, the public system, though free, is chronically underfunded and overcrowded. This model highlights a critical trade-off: privatization can drive medical advancements and reduce government spending, but it risks leaving vulnerable populations behind. For instance, a 2018 study found that Chilean women with private insurance were 50% more likely to receive timely cancer screenings compared to those relying on public services. Such disparities raise ethical concerns about prioritizing profit over public health.
From a practical standpoint, privatization can also lead to fragmented care. In the United States, where private hospitals dominate, patients often face higher out-of-pocket costs and a lack of coordination between providers. For example, a patient with diabetes might see an endocrinologist, a dietitian, and a primary care physician, each billing separately and potentially duplicating tests. This not only increases costs but also complicates patient management. In contrast, public systems like Canada’s often emphasize integrated care, where a single provider network coordinates services, reducing redundancy and improving outcomes. Policymakers considering privatization must weigh these operational challenges against potential benefits.
Advocates argue that private models foster competition, driving down costs and improving quality. However, this assumes a well-regulated market, which is rarely the case. In India, for instance, private hospitals often charge exorbitant fees for services, with some studies showing that up to 30% of households face catastrophic health expenditures due to private care. To mitigate such risks, governments must implement robust oversight, including price caps and quality standards. For example, Germany’s mixed system combines public insurance with private providers, ensuring affordability while maintaining high standards through strict regulations. Such balanced approaches offer lessons for countries navigating the privatization debate.
Ultimately, the privatization of healthcare is a double-edged sword. While it can alleviate financial burdens on public systems and introduce efficiencies, it also risks exacerbating inequalities and fragmenting care. Policymakers must carefully consider the societal impact, ensuring that any shift to private models includes safeguards for accessibility and equity. Practical steps include mandating transparency in pricing, subsidizing private care for low-income groups, and investing in public infrastructure to maintain a safety net. Without such measures, the move toward privatization could deepen healthcare disparities, leaving the most vulnerable further behind.
Medicare Hospital Stays: The 100-Day Limit Explained
You may want to see also
Explore related products






![]()
Cost of treatment: High medical expenses and their effect on accessibility and patient outcomes
High medical expenses are a barrier to healthcare access, disproportionately affecting low-income individuals and families. For instance, a 2020 study by the Kaiser Family Foundation found that 46% of U.S. adults reported difficulty paying medical bills, with one in five owing more than $5,000. These costs often stem from inflated drug prices, administrative overhead, and profit-driven practices within the healthcare system. A prime example is insulin, a life-saving medication for diabetics, which can cost up to $300 per vial in the U.S., compared to $30 in Canada. Such disparities highlight how capitalism in healthcare prioritizes profit over patient need, leaving many to choose between treatment and financial stability.
Consider the ripple effects of high treatment costs on patient outcomes. Delayed or forgone care due to expense exacerbates chronic conditions, leading to poorer health and higher long-term costs. For example, a patient with hypertension who skips medication to save money risks complications like stroke or heart attack, which require far costlier interventions. Similarly, preventive services like cancer screenings are often deferred, resulting in late-stage diagnoses that are harder and more expensive to treat. This cycle of avoidance and deterioration underscores how financial barriers not only limit access but also worsen health outcomes, perpetuating inequality in healthcare.
To mitigate these effects, patients can take proactive steps to navigate the system. First, inquire about generic medication options, which can reduce costs by up to 85%. For example, choosing generic atorvastatin (Lipitor) for cholesterol management instead of the brand-name version can save hundreds annually. Second, explore financial assistance programs offered by hospitals or pharmaceutical companies; many provide discounts or waivers for eligible patients. Third, negotiate bills directly with providers—a 2019 survey found that 57% of patients who attempted negotiation succeeded in lowering their costs. These strategies, while not systemic solutions, empower individuals to manage expenses and improve access to necessary care.
Comparatively, countries with universal healthcare systems demonstrate how reducing financial barriers improves outcomes. In the U.K., where the NHS covers most medical expenses, cancer survival rates are higher for certain demographics than in the U.S., despite similar diagnostic technologies. This is partly because early detection and consistent treatment are more accessible. Contrastingly, the U.S. system, driven by profit motives, often leaves patients uninsured or underinsured, leading to delayed care and poorer health. This comparison suggests that decoupling healthcare from capitalism could enhance both accessibility and patient outcomes on a population level.
Ultimately, the high cost of treatment is not merely a financial issue but a moral one, as it determines who receives care and who is left behind. While individual strategies can help manage expenses, systemic reform is necessary to address the root causes of inaccessibility. Policymakers must prioritize affordability through measures like price controls on essential medications, expanded insurance coverage, and reduced administrative waste. Until then, the capitalist framework of healthcare will continue to compromise patient outcomes, reinforcing the notion that health is a privilege, not a right.
Houston Hospitals with Therapy Dogs: Healing Paws in Action
You may want to see also
Explore related products



$29.37 $41



![]()
Pharmaceutical influence: Drug companies' role in hospital operations and treatment protocols for profit
Pharmaceutical companies wield significant influence over hospital operations, often shaping treatment protocols in ways that prioritize profit over patient-centered care. Consider the case of statins, cholesterol-lowering drugs prescribed to millions annually. While guidelines recommend statins for high-risk patients (e.g., those with a history of heart attack or LDL cholesterol >190 mg/dL), drug companies have lobbied to expand eligibility criteria. This includes targeting individuals with lower risk profiles, such as adults over 40 with LDL levels as low as 70 mg/dL, despite limited evidence of long-term benefits for this group. Hospitals, often reliant on pharmaceutical partnerships for funding, adopt these broader protocols, increasing drug prescriptions and company revenues.
The integration of drug company representatives into hospital settings further blurs the line between medical decision-making and profit motives. Sales reps frequently provide hospitals with free samples, funding for equipment, and even continuing education credits for staff. In exchange, they gain access to physicians, influencing prescribing habits through targeted marketing. For instance, a study found that doctors who met with reps were more likely to prescribe newer, costlier medications (e.g., brand-name insulin at $300/vial) over equally effective, cheaper alternatives (e.g., generic insulin at $50/vial). This dynamic not only inflates healthcare costs but also raises ethical concerns about the independence of clinical practice.
Hospitals’ financial dependence on pharmaceutical partnerships can also distort treatment priorities. Drug companies often sponsor clinical trials or provide grants for research, steering hospitals toward adopting their products. For example, a hospital might prioritize using a specific chemotherapy drug in cancer treatment protocols because the manufacturer funds its oncology department. While such collaborations can advance medical innovation, they risk sidelining treatments that lack corporate backing, even if they are more cost-effective or better suited to patient needs. This imbalance underscores the capitalist underpinnings of hospital-pharmaceutical relationships.
To mitigate pharmaceutical influence, hospitals must adopt transparent practices and prioritize evidence-based care. One practical step is to establish strict policies limiting interactions between staff and drug reps, such as banning gifts or meals. Additionally, hospitals should invest in independent drug formularies, relying on unbiased research rather than industry-sponsored studies. Patients can also play a role by questioning prescriptions and requesting generic alternatives when appropriate. For instance, if prescribed a brand-name blood pressure medication ($100/month), inquire about a generic version ($20/month) with the same active ingredient. By fostering accountability and critical thinking, hospitals can reclaim their focus on patient welfare, even within a profit-driven system.
Navigating Oregon: Distance from Sheridan to Newberg & Providence Hospital
You may want to see also
Explore related products





![]()
Labor exploitation: Underpaid healthcare workers and its connection to capitalist hospital systems
Healthcare workers, the backbone of any medical system, often find themselves at the mercy of a capitalist model that prioritizes profit over people. This is particularly evident in the widespread issue of underpayment, where nurses, technicians, and support staff are compensated far below the value they generate. For instance, in the United States, certified nursing assistants (CNAs) earn a median wage of $15 per hour, despite their physically and emotionally demanding roles. Compare this to the billions in profits raked in by hospital corporations, and the disparity becomes glaringly exploitative. This wage gap isn’t just a number—it’s a symptom of a system that treats labor as a cost to minimize rather than a resource to value.
Consider the capitalist imperative to maximize shareholder returns. Hospitals, increasingly operated by for-profit entities, are incentivized to cut labor costs wherever possible. This often translates to understaffing, overworking, and underpaying employees. Take the case of a registered nurse in a for-profit hospital, who might handle twice the patient load of their counterpart in a non-profit setting, yet receive only marginal pay increases. Such practices not only degrade the quality of care but also perpetuate a cycle of burnout and turnover, further straining the workforce. The irony? Patients ultimately bear the cost through higher medical bills and reduced care standards.
To break this cycle, healthcare workers must organize and demand systemic change. Unions, for example, have proven effective in negotiating fair wages and better working conditions. In California, SEIU-UHW has secured minimum staffing ratios and wage increases for hospital workers, demonstrating the power of collective action. However, this is just one piece of the puzzle. Policymakers must also address the root issue by regulating hospital profit margins and reinvesting those funds into labor. For instance, capping administrative salaries and redirecting savings to frontline workers could create a more equitable distribution of resources.
The connection between underpaid healthcare workers and capitalist hospital systems isn’t just theoretical—it’s tangible in the lives of those who keep our healthcare systems running. A CNA working 12-hour shifts for barely above minimum wage, a phlebotomist juggling multiple jobs to make ends meet, or a nurse forced to moonlight to pay off student loans—these are not isolated cases but systemic outcomes. Until we challenge the profit-driven model that undervalues their labor, the exploitation will persist, undermining the very foundation of healthcare itself.
Kettering Hospital: Adventist Health's Legacy in Healthcare
You may want to see also
Frequently asked questions
Hospitals can operate within capitalist systems, especially in countries with privatized healthcare, where profit motives influence decision-making. However, not all hospitals are capitalist; many are non-profit, government-run, or community-based, prioritizing public health over profit.
In capitalist healthcare systems, hospitals may face pressure to maximize profits, which can sometimes lead to cost-cutting measures or prioritizing high-revenue services. However, regulations, ethical standards, and competition often balance these pressures to ensure quality care.
Yes, hospitals can operate outside of capitalism. In countries with socialized or universal healthcare, hospitals are often publicly funded and focus on providing equitable care to all citizens, regardless of profitability. Non-profit and charitable hospitals also operate without a profit motive.




![Profit - 3-DVD Set ( Jim Profit ) [ NON-USA FORMAT, PAL, Reg.2 Import - Germany ]](https://m.media-amazon.com/images/I/61wYcjWLT6L._AC_UY218_.jpg)

























