Pneumonia, an infection that inflames the air sacs in one or both lungs, raises questions about the necessity of hospitalization for all cases. While some individuals with mild pneumonia can be treated effectively at home with antibiotics and rest, others may require hospitalization due to factors such as age, underlying health conditions, severity of symptoms, and the type of pneumonia. Hospitalization is often necessary for high-risk groups, including the elderly, young children, and those with weakened immune systems, as it allows for close monitoring, intravenous antibiotics, oxygen therapy, and other supportive care to prevent complications and ensure recovery. Understanding when hospitalization is warranted is crucial for managing pneumonia effectively and reducing the risk of severe outcomes.
| Characteristics | Values |
|---|---|
| Does all pneumonia require hospitalization? | No, not all cases of pneumonia require hospitalization. |
| Factors influencing hospitalization | Severity of symptoms, age, underlying health conditions, and type of pneumonia. |
| Mild pneumonia (outpatient treatment) | Often treated at home with oral antibiotics, rest, and fluids. Common in healthy adults with community-acquired pneumonia (CAP). |
| Moderate to severe pneumonia (hospitalization) | Requires hospitalization for intravenous antibiotics, oxygen therapy, and monitoring. Common in the elderly, young children, immunocompromised individuals, or those with severe symptoms. |
| High-risk groups for hospitalization | Adults over 65, children under 2, pregnant women, and individuals with chronic conditions (e.g., COPD, diabetes, heart disease). |
| Types more likely to require hospitalization | Aspiration pneumonia, hospital-acquired pneumonia (HAP), and pneumonia caused by drug-resistant bacteria. |
| Common symptoms requiring hospitalization | High fever, difficulty breathing, low oxygen levels, confusion, or inability to keep fluids down. |
| Latest guidelines (e.g., CURB-65) | Scoring systems like CURB-65 assess severity in adults; scores ≥2 often indicate hospitalization. |
| Pediatric guidelines (e.g., WHO) | Children with severe symptoms (e.g., hypoxia, dehydration) or high-risk factors require hospitalization. |
| COVID-19-related pneumonia | Hospitalization rates vary based on vaccination status, age, and comorbidities; severe cases often require intensive care. |
| Global trends | Hospitalization rates are decreasing in some regions due to vaccination (e.g., pneumococcal vaccine) and improved outpatient management. |
| Prevention strategies | Vaccination (pneumococcal, flu, COVID-19), avoiding smoking, and managing chronic conditions reduce hospitalization risk. |
Explore related products






What You'll Learn
![]()
Outpatient Treatment Criteria
Not all pneumonia cases necessitate hospitalization, and outpatient treatment can be a viable option for many patients. The decision to manage pneumonia on an outpatient basis hinges on specific criteria that assess the severity of the illness and the patient’s overall health. Key factors include the patient’s age, comorbidities, and the presence of certain risk factors. For instance, healthy adults under 65 with mild symptoms, no chronic illnesses, and reliable access to care are often candidates for outpatient treatment. In contrast, individuals over 65, those with conditions like diabetes or heart disease, or those exhibiting severe symptoms such as high fever, confusion, or difficulty breathing typically require hospitalization.
Outpatient treatment protocols are well-defined and typically involve a combination of antibiotics and supportive care. For bacterial pneumonia, common antibiotics like amoxicillin (500–1000 mg every 8 hours) or doxycycline (100 mg twice daily) are prescribed based on the suspected pathogen and local resistance patterns. Viral pneumonia, often caused by influenza or respiratory syncytial virus (RSV), may not require antibiotics but can benefit from antiviral medications like oseltamivir (75 mg twice daily for 5 days) for influenza. Supportive measures include rest, hydration, and over-the-counter medications for fever and pain, such as acetaminophen (650 mg every 4–6 hours as needed).
A critical aspect of outpatient management is close monitoring to ensure the patient’s condition does not deteriorate. Patients should be educated on warning signs that warrant immediate medical attention, such as worsening shortness of breath, persistent high fever, or chest pain. Follow-up appointments within 48–72 hours are essential to assess treatment response. Telehealth consultations can be particularly useful for monitoring patients remotely, especially in rural or underserved areas. Caregivers should also be instructed on how to assist the patient, including ensuring medication adherence and providing a calm, restful environment.
Comparatively, outpatient treatment is cost-effective and reduces the burden on healthcare systems, but it requires strict adherence to guidelines. For example, the CURB-65 score (Confusion, Urea, Respiratory rate, Blood pressure, Age ≥65) is a widely used tool to stratify pneumonia severity. Scores of 0–1 generally indicate suitability for outpatient treatment, while scores ≥2 suggest hospitalization. Similarly, the Pneumonia Severity Index (PSI) categorizes patients into risk classes, with classes I–III often managed as outpatients. These tools, combined with clinical judgment, help providers make informed decisions tailored to the patient’s needs.
In practice, successful outpatient treatment relies on patient selection and clear communication. Providers must ensure patients understand their treatment plan and the importance of follow-up. Practical tips include keeping a symptom diary, using medication reminders, and having a reliable support system. For parents managing pediatric cases, ensuring children complete the full antibiotic course and monitoring for dehydration are crucial. By adhering to these criteria and strategies, outpatient treatment can effectively manage pneumonia while minimizing the need for hospitalization.
Annual Birth Rates at Mercy Hospital Portland: A Comprehensive Overview
You may want to see also
Explore related products






![]()
Severity Assessment Tools
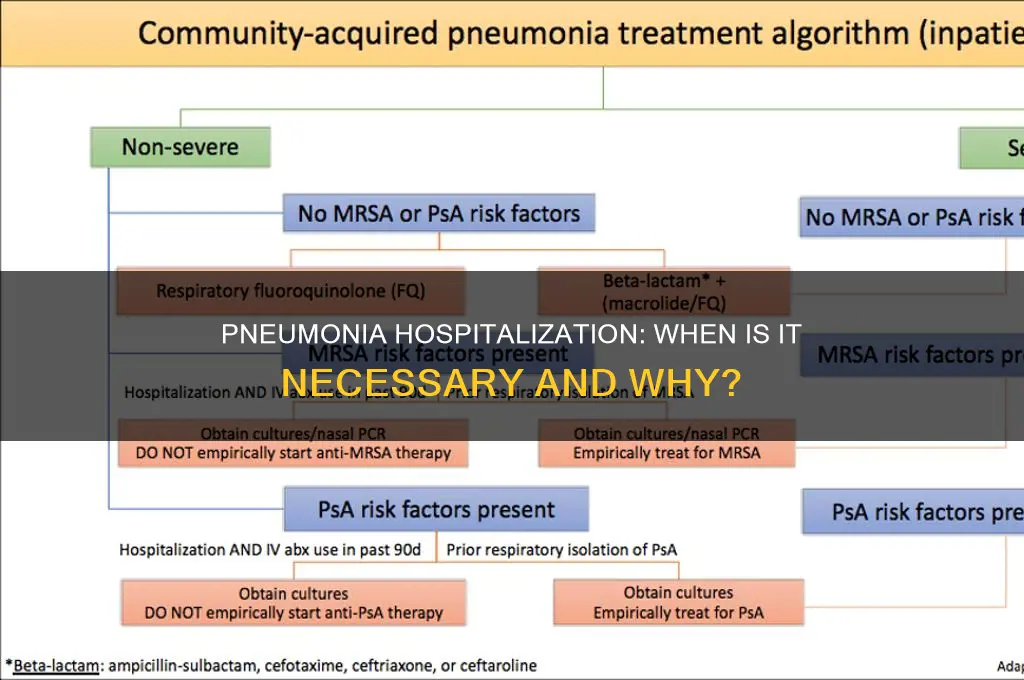
Not all pneumonia cases warrant hospitalization, and determining the appropriate level of care is crucial for patient outcomes and resource allocation. This is where severity assessment tools come into play, offering a structured approach to evaluate the risk and guide clinical decision-making. These tools are particularly valuable in emergency departments and primary care settings, where rapid triage is essential.
The CURB-65 Score: A Widely Adopted Tool
One of the most recognized severity assessment tools is the CURB-65 score, designed to predict mortality risk in community-acquired pneumonia (CAP). It assigns points based on five criteria: Confusion, Urea > 7 mmol/L, Respiratory rate ≥ 30 breaths/min, Blood pressure (systolic < 90 mmHg or diastolic ≤ 60 mmHg), and Age ≥ 65 years. Each criterion earns one point, except age, which is a binary factor. A total score of 0-1 suggests low risk, often manageable as an outpatient, while scores of 2 or higher indicate moderate to severe disease, potentially requiring hospitalization. For instance, a 70-year-old patient with a respiratory rate of 32 breaths/min, confusion, and a urea level of 8 mmol/L would score 4, strongly suggesting hospital admission.
Comparing Tools: CURB-65 vs. PSI/PORT Score
While CURB-65 is straightforward and widely used, the Pneumonia Severity Index (PSI) or PORT score offers a more comprehensive assessment. PSI categorizes patients into risk classes (I-V) based on age, comorbidities, physical examination findings, and laboratory data. This tool is more complex, requiring up to 20 variables, but it provides a nuanced prediction of 30-day mortality. For example, a 55-year-old with diabetes, a heart rate of 110 bpm, and a temperature of 39°C might fall into class III, indicating potential benefits from hospitalization. However, the complexity of PSI can limit its use in busy clinical settings, making CURB-65 a more practical choice for quick decisions.
Implementing Tools in Clinical Practice
To effectively use severity assessment tools, healthcare providers should follow a structured approach. First, gather all necessary data points, ensuring accuracy in measurements like respiratory rate and blood pressure. Second, calculate the score promptly, especially in high-volume settings. Third, interpret the results in the context of the patient’s overall health and available resources. For instance, a CURB-65 score of 2 in a frail elderly patient might warrant hospitalization, even if the score alone suggests intermediate risk. Additionally, consider local guidelines and antibiotic stewardship programs to optimize care.
Limitations and Future Directions
Despite their utility, severity assessment tools are not without limitations. They rely on clinical and laboratory data, which may not always be immediately available. Moreover, they do not account for patient preferences or social determinants of health, which can significantly impact treatment decisions. Emerging technologies, such as machine learning algorithms, may enhance these tools by incorporating real-time data and personalized factors. For now, clinicians should use these tools as aids, not replacements for clinical judgment, ensuring a holistic approach to pneumonia management.
Leading Cancer Hospitals in America: Where to Turn?
You may want to see also
Explore related products

$17.98 $19.99





![]()
Risk Factors for Hospitalization
Not all pneumonia cases demand hospital admission, but certain risk factors significantly increase the likelihood of hospitalization. Age stands as a primary determinant: individuals over 65 and children under 5 face higher risks due to weaker immune systems. For instance, older adults often have comorbidities like diabetes or heart disease, which complicate pneumonia management at home. Similarly, infants and young children may struggle to fight infections effectively, necessitating closer medical monitoring.
Severity of symptoms also plays a critical role in hospitalization decisions. High fever (above 102°F or 39°C), persistent cough with pus-like mucus, and difficulty breathing are red flags. Oxygen saturation levels below 90% indicate respiratory distress, often requiring immediate hospital intervention. For example, a patient with a rapid breathing rate (over 30 breaths per minute) and chest retractions may need supplemental oxygen, which is typically administered in a clinical setting.
Underlying health conditions amplify the risk of hospitalization. Chronic lung diseases like COPD or asthma, weakened immune systems (e.g., from HIV or chemotherapy), and neurological disorders affecting swallowing increase susceptibility to severe pneumonia. For instance, patients with COPD are 2-3 times more likely to be hospitalized for pneumonia compared to those without. Additionally, smokers and individuals with alcohol use disorder face heightened risks due to compromised lung function and immune response.
Environmental and lifestyle factors further contribute to hospitalization risks. Exposure to air pollution, crowded living conditions, and lack of access to healthcare increase vulnerability. For example, individuals in long-term care facilities are at higher risk due to close contact with others and potential exposure to antibiotic-resistant strains. Practical tips include annual flu and pneumococcal vaccinations, especially for high-risk groups, and avoiding smoking or secondhand smoke to reduce lung inflammation.
Finally, the causative pathogen can influence hospitalization rates. Bacterial pneumonia, particularly from *Streptococcus pneumoniae*, often requires intravenous antibiotics and hospital care. Viral pneumonia, while sometimes milder, can progress rapidly in immunocompromised individuals. Atypical pathogens like *Mycoplasma pneumoniae* may cause severe symptoms in children and young adults, necessitating hospitalization. Understanding these risk factors helps healthcare providers make informed decisions, ensuring timely and appropriate care for pneumonia patients.
Who Leads Code Blue? Anesthesiologist's Role in Hospital Resuscitation
You may want to see also
Explore related products






![]()
Home Management Strategies
Not all pneumonia cases demand hospital admission. For mild to moderate bacterial pneumonia in otherwise healthy adults, home management is often feasible. This approach hinges on timely diagnosis, access to appropriate antibiotics, and vigilant monitoring for deterioration. Oral antibiotics like amoxicillin (500 mg three times daily for 7-10 days) or doxycycline (100 mg twice daily for 7 days) are typically prescribed based on suspected pathogen and regional resistance patterns. Adherence to the full course is critical, even if symptoms improve within 48-72 hours.
Effective home management requires a structured symptom-monitoring protocol. Patients should track oxygen saturation (target ≥92% on room air), respiratory rate (<24 breaths/minute in adults), and temperature daily. Any persistent fever beyond 48 hours of treatment, worsening shortness of breath, or oxygen saturation below 90% necessitates immediate medical re-evaluation. Hydration is paramount—aim for 2-3 liters of fluid daily to thin secretions and aid expectoration. Incentive spirometry (8-10 breaths every 2 hours) helps prevent lung atelectasis, particularly in elderly patients or those with prolonged bed rest.
Pain management is often overlooked but essential for adequate coughing and secretion clearance. Acetaminophen (650-1000 mg every 6 hours) or ibuprofen (400-600 mg every 6 hours) can alleviate pleuritic chest pain, but caution is advised in patients with renal impairment or gastrointestinal risks. Guaifenesin (600 mg every 12 hours) may assist in expectoration, though evidence is limited. Humidified air (via a cool-mist humidifier) and steam inhalation (10-15 minutes twice daily) can soothe bronchial irritation and loosen mucus.
Pediatric cases warrant special considerations. Children under 5 years, particularly those with hypoxia or dehydration, often require hospitalization. For those managed at home, caregivers must monitor for signs of respiratory distress (e.g., nasal flaring, grunting, or retractions) and ensure age-appropriate antibiotic dosing (e.g., amoxicillin 40-50 mg/kg/day divided twice daily). Oral rehydration solutions (5-10 mL/kg per hour) are critical for infants with poor fluid intake.
Successful home management relies on patient education and a clear escalation plan. Patients should understand red flags (e.g., confusion, bluish lips, inability to tolerate oral intake) and have immediate access to medical advice. Follow-up within 48-72 hours of initiating treatment is standard to assess clinical response. While home care is viable for selected cases, it is not a substitute for hospital-level care in severe pneumonia, particularly in immunocompromised individuals, the elderly, or those with comorbidities like COPD or diabetes.
High Fever in 10-Year-Olds: When to Seek Hospital Care
You may want to see also
Explore related products






![]()
Complications Requiring Admission
Not all pneumonia cases demand hospitalization, but certain complications can swiftly escalate the need for inpatient care. Respiratory distress, marked by rapid breathing (tachypnea), hypoxia (oxygen saturation below 90%), or retractions, signals a critical condition that outpatient management cannot address. For instance, a 65-year-old patient with tachypnea (>30 breaths/min) and SpO₂ of 88% on room air requires immediate admission for supplemental oxygen and close monitoring. This scenario underscores the importance of recognizing early signs of respiratory failure, which, if left untreated, can progress to acute respiratory distress syndrome (ARDS).
Sepsis, another red-flag complication, necessitates hospitalization when pneumonia triggers systemic inflammation and organ dysfunction. Hypotension (systolic blood pressure <90 mmHg) or the need for vasopressors, along with altered mental status or lactic acidosis (>4 mmol/L), are criteria that mandate admission. For example, a 45-year-old diabetic patient with pneumonia, a heart rate of 110 bpm, and confusion should be evaluated for septic shock. Early administration of intravenous antibiotics, such as ceftriaxone (1g every 24 hours) plus azithromycin (500 mg daily), coupled with fluid resuscitation, can prevent mortality in such cases.
In pediatric populations, dehydration due to poor oral intake or persistent high fever (>39°C) often complicates pneumonia and requires hospitalization. A 2-year-old with severe dehydration, characterized by sunken eyes and reduced urine output, may need intravenous fluids (20 mL/kg bolus of normal saline) to stabilize. Similarly, children under 5 years old with severe pneumonia, defined by WHO criteria (e.g., chest indrawing), should be admitted for oxygen therapy and antibiotics like ampicillin (50 mg/kg every 6 hours). These interventions highlight the age-specific thresholds for inpatient care.
Finally, comorbidities such as chronic obstructive pulmonary disease (COPD), congestive heart failure, or immunocompromised states (e.g., HIV, chemotherapy) amplify the risk of complications. A 70-year-old COPD patient with pneumonia and worsening hypercapnia (PaCO₂ >50 mmHg) may develop respiratory acidosis, necessitating noninvasive ventilation (NIV) in a hospital setting. Practical tips include monitoring for subtle signs like increased sputum production or weight gain (>3 lbs in 2 days) in heart failure patients, which could indicate fluid overload. Admission in these cases ensures tailored management, preventing decompensation of underlying conditions.
In summary, while mild pneumonia can be managed outpatient, complications like respiratory distress, sepsis, dehydration, and exacerbation of comorbidities require hospitalization. Recognizing these red flags and initiating prompt, evidence-based interventions can significantly improve outcomes. Always assess individual risk factors and clinical severity to determine the appropriate level of care.
Opening an Animal Hospital: Pennsylvania's Guide
You may want to see also
Frequently asked questions
No, not all pneumonia cases require hospitalization. Mild to moderate cases, especially in otherwise healthy individuals, can often be treated at home with oral antibiotics and rest.
Individuals with severe symptoms, the elderly, young children, those with weakened immune systems, or people with underlying health conditions like heart or lung disease are more likely to require hospitalization.
Symptoms such as high fever, difficulty breathing, low oxygen levels, confusion, persistent chest pain, or inability to keep fluids down often indicate the need for hospitalization.
Yes, many cases of pneumonia can be treated at home with proper medical guidance, including antibiotics, rest, hydration, and over-the-counter pain relievers. However, severe cases or high-risk individuals should seek medical evaluation.