Compartment syndrome is a serious medical condition that occurs when excessive pressure builds up within a muscle compartment, compromising blood flow and potentially leading to muscle and nerve damage. When this condition is suspected, immediate hospitalization is crucial for diagnosis and treatment. In the hospital, healthcare providers typically perform a thorough physical examination, assess symptoms such as severe pain, swelling, and tightness in the affected limb, and may use tools like compartment pressure measurements to confirm the diagnosis. Treatment often involves emergency fasciotomy, a surgical procedure to relieve pressure by cutting open the fascia surrounding the affected compartment, preventing permanent tissue damage and restoring blood flow. Prompt hospital intervention is essential to prevent long-term complications, including muscle necrosis, nerve dysfunction, and potential limb loss.
| Characteristics | Values |
|---|---|
| Definition | Compartment syndrome is a painful condition caused by increased pressure within a confined space in the body, often in the leg, arm, or abdomen, leading to impaired blood flow and potential muscle and nerve damage. |
| Causes | Trauma (e.g., fractures, crush injuries), prolonged compression, excessive swelling, tight bandages or casts, vigorous exercise, and certain medical conditions (e.g., bleeding disorders). |
| Symptoms | Severe pain (disproportionate to the injury), tightness or fullness in the affected area, numbness or tingling, weakness, pale or bluish skin, and difficulty moving the affected limb. |
| Diagnosis | Clinical assessment, measurement of compartment pressure (intracompartmental pressure > 30 mmHg or within 30 mmHg of diastolic blood pressure), and imaging (e.g., MRI, CT scan) if necessary. |
| Treatment | Emergency fasciotomy: Surgical release of the compartment to relieve pressure. Delayed treatment can lead to permanent muscle and nerve damage, amputation, or even death. |
| Hospital Management | Immediate admission to the emergency department, continuous monitoring of vital signs, pain management, elevation of the affected limb (if applicable), and urgent surgical consultation. |
| Prevention | Proper casting and bandaging techniques, early recognition of symptoms, and prompt medical attention after injuries. |
| Complications | Volkmann’s contracture, muscle necrosis, nerve damage, kidney failure (rhabdomyolysis), disability, and limb loss if untreated. |
| Prognosis | Good if treated promptly; poor outcomes if treatment is delayed, leading to permanent functional impairment or loss of limb. |
| Latest Research | Focus on early diagnosis tools, minimally invasive treatments, and improved surgical techniques to reduce complications and improve recovery. |
Explore related products






What You'll Learn
- Diagnosis Methods: Physical exams, pressure measurements, and imaging tests identify compartment syndrome quickly
- Immediate Treatment: Fasciotomy surgery is crucial to relieve pressure and prevent tissue damage
- Post-Surgery Care: Monitoring, wound management, and physical therapy aid recovery after fasciotomy
- Risk Factors: Trauma, fractures, burns, and prolonged compression increase compartment syndrome likelihood
- Long-Term Effects: Untreated cases can lead to muscle necrosis, nerve damage, or limb loss
![]()
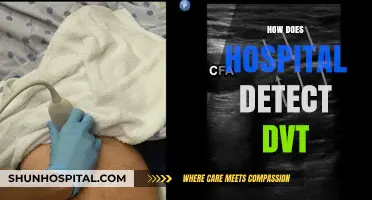
Diagnosis Methods: Physical exams, pressure measurements, and imaging tests identify compartment syndrome quickly
Compartment syndrome demands swift diagnosis to prevent irreversible damage. Physical exams serve as the frontline tool, with clinicians assessing pain disproportionate to findings, passive stretch pain, and tense compartmental swelling. A high index of suspicion is crucial, especially in high-risk scenarios like traumatic fractures, crush injuries, or prolonged limb compression. For instance, a patient with a tibial fracture complaining of severe pain unrelieved by opioids warrants immediate evaluation.
Pressure measurements, particularly intracompartmental pressure (ICP) monitoring, provide objective data to confirm suspicion. Normal resting ICP is below 10 mmHg, while pressures exceeding 30 mmHg or a pressure gradient (delta pressure) below 30 mmHg between diastolic blood pressure and ICP indicate critical compartment syndrome. Continuous monitoring may be necessary in equivocal cases, as pressures can fluctuate. However, this method requires specialized equipment and expertise, limiting its accessibility in resource-constrained settings.
Imaging tests, though not definitive, play a supportive role in diagnosis. MRI can detect edema and muscle necrosis but is time-consuming and impractical in emergencies. Ultrasound, on the other hand, offers real-time visualization of muscle swelling, fascial thickening, and fluid accumulation, aiding in early detection. For example, a point-of-care ultrasound in a patient with forearm compartment syndrome may reveal hypoechoic muscle tissue and distended vessels, corroborating clinical suspicion.
The interplay of these methods underscores the importance of a multimodal approach. Physical exams provide immediacy, pressure measurements offer objectivity, and imaging tests enhance diagnostic confidence. Clinicians must act decisively, as delays in diagnosis can lead to muscle ischemia, nerve damage, and functional loss. For instance, a delayed diagnosis in a young athlete with exertional compartment syndrome could result in career-ending complications.
In practice, a structured protocol is essential. Begin with a thorough physical exam, proceed to ICP measurement if suspicion is high, and incorporate imaging to rule out differential diagnoses. Education of emergency and surgical teams is critical, as compartment syndrome often presents in acute care settings. By integrating these methods, hospitals can ensure timely intervention, preserving limb function and patient outcomes.
Cleveland Clinic in Florida: Where and What?
You may want to see also
Explore related products






![]()
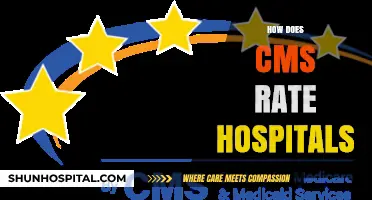
Immediate Treatment: Fasciotomy surgery is crucial to relieve pressure and prevent tissue damage
Compartment syndrome, a condition where increased pressure within a muscle compartment compromises blood flow, demands immediate intervention to prevent irreversible damage. Among the critical treatments, fasciotomy surgery stands out as the definitive solution to relieve pressure and restore circulation. This procedure involves cutting open the fascia, the connective tissue surrounding muscle groups, to decompress the affected area. Without prompt fasciotomy, patients risk muscle necrosis, nerve damage, and even limb loss, underscoring its urgency in the hospital setting.
The decision to perform a fasciotomy is guided by clinical judgment and objective measurements. Key indicators include severe pain disproportionate to findings on physical examination, pain with passive stretching of the muscles, and signs of impaired circulation such as pallor, paresthesia, or pulselessness. Intracompartmental pressure monitoring, though not always necessary, can confirm the diagnosis when clinical suspicion is high. Once compartment syndrome is suspected, surgery should be performed within hours, as delays beyond 6–12 hours significantly worsen outcomes.
During the fasciotomy, surgeons make longitudinal incisions through the skin and fascia to expose the affected compartment. The procedure is often performed under general or regional anesthesia, with careful attention to avoiding further tissue trauma. Postoperatively, patients require close monitoring for complications such as infection or bleeding, and the wounds are typically left open for 48–72 hours to ensure adequate decompression. Subsequent wound closure may involve skin grafting or delayed primary closure, depending on tissue viability.
While fasciotomy is highly effective, it is not without risks. Surgical site infections, scarring, and functional deficits can occur, particularly in patients with preexisting conditions like diabetes or peripheral vascular disease. However, the benefits of preventing permanent disability far outweigh these risks. Early recognition and swift action remain the cornerstones of successful management, making fasciotomy an indispensable tool in the hospital’s arsenal against compartment syndrome.
Texas Hospitals: Citizenship Question Under Scrutiny
You may want to see also
Explore related products






![]()
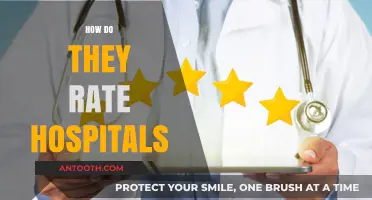
Post-Surgery Care: Monitoring, wound management, and physical therapy aid recovery after fasciotomy
Compartment syndrome, a condition where increased pressure within a muscle compartment compromises blood flow, often necessitates a fasciotomy—a surgical procedure to relieve pressure. Post-surgery care is critical to ensure proper healing, prevent complications, and restore function. Monitoring, wound management, and physical therapy form the cornerstone of this recovery process, each playing a distinct yet interconnected role in the patient’s journey.
Monitoring: Vigilance in the Early Stages
Immediate post-operative monitoring is paramount to detect any signs of recurrent compartment syndrome or infection. Vital signs, including blood pressure, heart rate, and oxygen saturation, are tracked hourly for the first 24 hours, then gradually reduced as stability is confirmed. Wound drainage and swelling are closely observed, with any sudden increase in pain or numbness warranting immediate medical attention. For high-risk patients, such as athletes or those with traumatic injuries, continuous compartment pressure monitoring may be employed, though this is less common post-fasciotomy. Early detection of complications can significantly reduce the risk of reoperation or long-term disability.
Wound Management: Precision in Healing
Fasciotomy wounds are typically left open initially to prevent pressure buildup, requiring meticulous care to avoid infection and promote healing. Dressings are changed daily using sterile technique, with antimicrobial solutions like povidone-iodine or chlorhexidine applied to reduce bacterial load. Once swelling subsides, usually within 48–72 hours, the wound is closed surgically or via delayed primary closure. Patients are instructed to keep the area clean and dry, avoiding strenuous activity that could disrupt sutures. For open wounds, negative pressure wound therapy (NPWT) may be utilized to enhance healing, particularly in cases of extensive tissue damage. Adherence to wound care protocols is essential to minimize scarring and ensure functional recovery.
Physical Therapy: Restoring Strength and Mobility
Physical therapy begins as soon as the patient’s condition stabilizes, often within days of surgery. Initial focus is on gentle range-of-motion exercises to prevent joint stiffness, such as ankle pumps or wrist flexions, performed 3–5 times daily. As healing progresses, resistance exercises are introduced to rebuild muscle strength, starting with light resistance bands and advancing to weights. Patients are cautioned against overexertion, as premature stress on the surgical site can lead to complications. For lower extremity fasciotomies, gait training with assistive devices like crutches or walkers is incorporated to ensure safe ambulation. A structured, progressive therapy plan tailored to the individual’s needs accelerates recovery and improves long-term outcomes.
Integration of Care: A Holistic Approach
Effective post-fasciotomy recovery requires seamless integration of monitoring, wound management, and physical therapy. Interdisciplinary collaboration between surgeons, nurses, and physical therapists ensures that each aspect of care is addressed comprehensively. Patient education is equally vital; individuals must understand the importance of adhering to wound care instructions, attending therapy sessions, and recognizing warning signs of complications. By combining vigilance, precision, and rehabilitation, healthcare providers can optimize recovery and help patients regain functionality after this life-altering procedure.
Are US Hospitals Federally Mandated? Exploring Healthcare Regulations and Oversight
You may want to see also
Explore related products






![]()
Risk Factors: Trauma, fractures, burns, and prolonged compression increase compartment syndrome likelihood
Trauma stands as a primary catalyst for compartment syndrome, often setting off a chain reaction within the body’s fascial compartments. High-energy injuries, such as those from car accidents or falls, can cause direct muscle damage, bleeding, or swelling, rapidly elevating pressure within these confined spaces. For instance, a tibial fracture in the lower leg can lead to bleeding from torn blood vessels, accumulating hematoma, and subsequent compartment pressure spikes. Hospitals must act swiftly in trauma cases, monitoring for signs like severe pain disproportionate to the injury, tightness in the affected limb, or decreased pulses, which may necessitate emergency fasciotomy to prevent irreversible muscle and nerve damage.
Fractures, particularly those involving long bones like the femur or tibia, pose a significant risk due to their potential to cause immediate compartmental compromise. Even closed fractures can lead to swelling and bleeding within the compartment, while open fractures introduce additional risks of infection and tissue disruption. A study in *The Journal of Bone and Joint Surgery* highlights that up to 5% of tibial fractures develop compartment syndrome, emphasizing the need for vigilant monitoring. Clinicians should assess fracture patients regularly, especially within the first 24–48 hours post-injury, and consider compartment pressure measurements if symptoms arise, as delayed intervention can lead to limb-threatening complications.
Burns, especially circumferential burns involving limbs, create a unique risk profile for compartment syndrome due to their systemic and local effects. The inflammatory response to burns causes fluid shifts and edema, which can increase compartment pressure, particularly in the lower legs and arms. For example, a third-degree circumferential leg burn can lead to eschar formation, a hardened layer of dead tissue that acts like a cast, restricting tissue expansion and exacerbating pressure. Burn units often employ escharotomies—surgical incisions through the eschar—to relieve pressure and prevent compartment syndrome. Early recognition and intervention are critical, as burn patients may already be compromised by fluid resuscitation and systemic inflammation.
Prolonged compression, often overlooked, can silently contribute to compartment syndrome, particularly in vulnerable populations like the elderly, immobilized patients, or those under general anesthesia. For instance, a patient lying in one position for hours during surgery may develop compartment syndrome in a limb due to sustained pressure on muscles and nerves. Similarly, tight casts or dressings applied post-injury can restrict circulation and elevate compartment pressure if not monitored. Hospitals should educate staff on proper positioning techniques, regularly assess patients for signs of compression-related issues, and ensure casts are split or adjusted if swelling occurs. Prevention here is key, as prolonged compression often goes unnoticed until irreversible damage occurs.
In summary, trauma, fractures, burns, and prolonged compression are critical risk factors for compartment syndrome, each requiring tailored vigilance and intervention. Hospitals must adopt a proactive approach, from immediate trauma assessments to post-operative positioning protocols, to mitigate these risks. Early recognition, coupled with timely surgical intervention when necessary, remains the cornerstone of preventing the devastating consequences of this condition. By understanding these specific risk factors, healthcare providers can better protect patients and improve outcomes in high-risk scenarios.
Detecting Kidney Stones: Hospital Diagnostics and Imaging Techniques
You may want to see also
Explore related products


![The Syndrome [DVD]](https://m.media-amazon.com/images/I/51tZKS1u6nL._AC_UY218_.jpg)



![]()
Long-Term Effects: Untreated cases can lead to muscle necrosis, nerve damage, or limb loss
Compartment syndrome, if left untreated, can escalate into a medical emergency with devastating consequences. The condition arises when pressure within a muscle compartment increases, compromising blood flow and oxygen delivery to tissues. Without prompt intervention, this ischemia progresses, leading to irreversible damage. Understanding the long-term effects—muscle necrosis, nerve damage, and potential limb loss—underscores the urgency of early diagnosis and treatment.
Consider the mechanism: as pressure builds within a compartment, it surpasses capillary perfusion pressure, causing cellular ischemia. Within hours, muscle and nerve cells begin to die. For instance, muscle necrosis can occur as early as 4–6 hours after the onset of ischemia, while nerve damage may manifest within 8–12 hours. These timelines are not rigid but highlight the rapid deterioration possible in untreated cases. Practical tip: monitor for the "5 Ps" of compartment syndrome—pain, pallor, paresthesia, pulselessness, and paralysis—and seek immediate medical attention if symptoms persist or worsen.
Comparatively, the outcomes of untreated compartment syndrome are far more severe than those of timely intervention. Fasciotomy, the gold-standard treatment, involves surgically releasing the compartment pressure to restore blood flow. Delayed treatment, however, often results in irreversible tissue damage. For example, a study published in *The Journal of Bone and Joint Surgery* found that fasciotomy performed within 8 hours of symptom onset significantly reduced the risk of muscle necrosis and nerve damage compared to later interventions. Caution: even with surgery, patients who present late may still face long-term disabilities, including chronic pain, reduced mobility, and sensory deficits.
Persuasively, the long-term effects of untreated compartment syndrome extend beyond physical impairment to impact quality of life. Limb loss, though a worst-case scenario, is a stark reality for some patients. Amputation rates are higher in cases where diagnosis and treatment are delayed, particularly in high-risk populations such as trauma patients, athletes, and those with casts or tight dressings. For instance, a 2019 review in *Orthopaedic Nursing* emphasized that early recognition and intervention could prevent up to 70% of amputations related to compartment syndrome. Practical advice: educate at-risk individuals about the signs of compartment syndrome and the importance of not ignoring persistent or worsening symptoms.
Descriptively, the progression from untreated compartment syndrome to long-term complications is a grim but preventable trajectory. Imagine a scenario where a patient with a fractured tibia experiences increasing pain and swelling. Without timely fasciotomy, the compartment pressure continues to rise, cutting off blood supply. Days later, the patient presents with a pale, pulseless limb, and despite emergency surgery, muscle necrosis has already set in. Over months, they may undergo multiple debridements, skin grafts, or even amputation, followed by years of rehabilitation. This outcome is not inevitable—early intervention can halt the cascade of damage and preserve function. Takeaway: compartment syndrome is a time-sensitive condition where every hour counts. Recognize the signs, act swiftly, and advocate for immediate medical care to prevent life-altering consequences.
Batman's Brutal Vigilantism: Hospitalizing Criminals in Gotham City
You may want to see also
Frequently asked questions
Compartment syndrome is a painful condition caused by increased pressure within a muscle compartment, often due to injury, swelling, or bleeding. It requires immediate hospitalization for diagnosis and treatment to prevent muscle and nerve damage.
Symptoms include severe pain, especially when moving the affected limb, tightness or swelling in the muscle, numbness or tingling, and pale or bluish skin. These symptoms necessitate urgent medical attention and hospitalization.
Diagnosis involves a physical exam, measuring compartment pressure using a needle or specialized device, and assessing symptoms. Imaging tests like X-rays or MRI may also be used to rule out other conditions.
Immediate treatment includes surgery (fasciotomy) to relieve pressure in the compartment. Pain management, elevation of the limb, and monitoring for complications are also part of hospital care.
Delaying treatment can lead to permanent muscle and nerve damage, loss of function in the affected limb, and in severe cases, amputation or life-threatening complications like kidney failure due to rhabdomyolysis.