Detecting deep vein thrombosis (DVT) in a hospital setting involves a combination of clinical assessment, diagnostic tools, and laboratory tests. Healthcare providers typically begin by evaluating symptoms such as swelling, pain, warmth, and redness in the affected limb, often accompanied by a thorough medical history to identify risk factors like recent surgery, immobility, or a history of blood clots. The primary diagnostic test is compression ultrasound, which uses sound waves to visualize blood flow and detect clots in the deep veins. In some cases, a D-dimer blood test may be performed to rule out DVT, though it is less specific and often used in conjunction with other methods. Additional imaging techniques, such as venography or CT scans, may be employed if ultrasound results are inconclusive. Early and accurate detection is crucial to prevent potentially life-threatening complications, such as pulmonary embolism, and to initiate prompt treatment with anticoagulant therapy.
Explore related products



![[2025 VER] Hidden Device Detector, Hidden Camera Detectors with Vibration Sound Alarm, Camera Finder with Flashlight, GPS Tracker Detector for Car, Listening Device Detector for Office, 1 Pack](https://m.media-amazon.com/images/I/61TU93VriXL._AC_UY218_.jpg)


What You'll Learn
- Ultrasound Imaging: Uses Doppler to visualize blood flow and clot presence in veins
- D-Dimer Blood Test: Detects fibrin degradation, indicating possible clot breakdown in the body
- Venography: Injects contrast dye to highlight clots in vein X-rays
- Physical Examination: Checks for swelling, warmth, and redness in affected limbs
- Risk Factor Assessment: Evaluates medical history, surgery, immobility, and genetic predisposition
![]()
Ultrasound Imaging: Uses Doppler to visualize blood flow and clot presence in veins
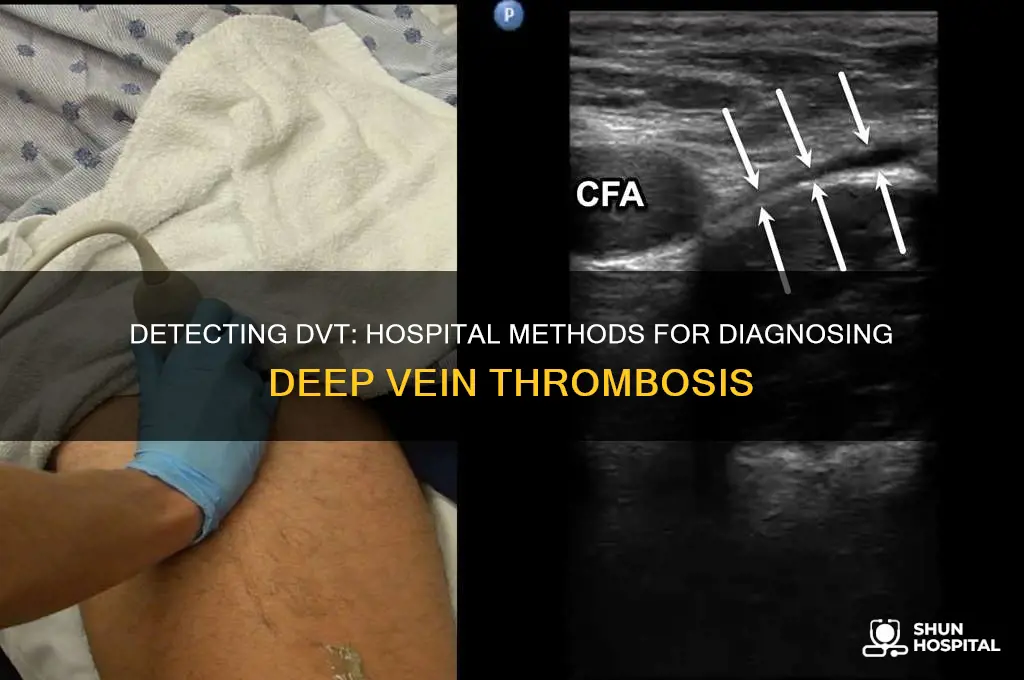
Deep vein thrombosis (DVT) diagnosis hinges on ultrasound imaging, a non-invasive technique that leverages Doppler technology to assess blood flow and detect clots within veins. Unlike static X-rays, ultrasound provides dynamic, real-time visualization of venous structures, making it the gold standard for DVT detection. The procedure involves a transducer emitting high-frequency sound waves that penetrate the skin, bounce off blood cells, and return as echoes. These echoes are processed to create images of the veins, with Doppler enhancing the visualization by measuring the direction and speed of blood flow. This dual capability allows clinicians to identify obstructions indicative of a clot.
The process begins with the application of a water-based gel to the skin, which eliminates air pockets and ensures optimal sound wave transmission. The technician then moves the transducer along the suspected area, typically the legs, capturing images of the femoral, popliteal, and calf veins. Doppler technology distinguishes between normal laminar flow and turbulent or absent flow, which may suggest a clot. For instance, a complete absence of flow in a vein segment, coupled with an expanded vein diameter, strongly indicates DVT. Partial clots may show reduced flow velocity or irregular patterns, requiring further evaluation.
One of the key advantages of ultrasound is its ability to differentiate between acute and chronic clots. Acute clots often appear as echogenic (bright) masses within the vein, while chronic clots may be less distinct or adhered to the vein wall. Additionally, Doppler can detect collateral circulation, where blood reroutes around a blocked vein, a sign of long-standing DVT. This distinction is crucial for treatment planning, as acute clots may require immediate anticoagulation, whereas chronic cases might focus on preventing complications like post-thrombotic syndrome.
Despite its efficacy, ultrasound has limitations. Operator dependency is a significant factor, as the quality of the images relies on the technician’s skill and experience. Suboptimal imaging can lead to false negatives, particularly in small or deep veins. To mitigate this, hospitals often employ compression ultrasound, where the technician applies gentle pressure to the vein. If the vein compresses fully, DVT is unlikely; if it remains non-compressible, a clot is confirmed. This technique enhances diagnostic accuracy, especially in challenging cases.
In practice, ultrasound is often the first-line imaging modality for DVT due to its accessibility, speed, and lack of radiation exposure. It is particularly valuable in emergency settings, where rapid diagnosis is critical. For patients with contraindications to other imaging methods, such as contrast allergies or renal impairment, ultrasound offers a safe alternative. However, in complex cases or when ultrasound results are inconclusive, clinicians may opt for additional tests like CT venography or MRI. Nonetheless, for most patients, ultrasound remains the cornerstone of DVT detection, combining precision with practicality.
Adventist Health Hospital Fort Bragg: Accepted Insurance Plans Guide
You may want to see also
Explore related products






![]()
D-Dimer Blood Test: Detects fibrin degradation, indicating possible clot breakdown in the body
Deep vein thrombosis (DVT) is a serious condition where blood clots form in deep veins, often in the legs. Detecting it early is crucial to prevent life-threatening complications like pulmonary embolism. One of the key tools hospitals use is the D-Dimer blood test, which detects fibrin degradation products—a telltale sign of clot breakdown in the body. This test is non-invasive, quick, and serves as an initial screening tool to rule out DVT in low-risk patients. However, its effectiveness hinges on understanding its limitations and proper interpretation.
The D-Dimer test measures the concentration of D-Dimer proteins in the blood, which are released when fibrin clots are broken down by plasmin. Elevated levels suggest clotting activity, but the test is not specific to DVT. High D-Dimer levels can also indicate other conditions like infection, inflammation, or recent surgery. For this reason, the test is often used in conjunction with clinical assessment tools like the Wells score, which evaluates symptoms and risk factors to determine the likelihood of DVT. A negative D-Dimer result in a low-risk patient can effectively rule out DVT, avoiding the need for further imaging studies.
Performing the D-Dimer test is straightforward. A healthcare provider draws a small blood sample, typically from a vein in the arm, and sends it to the lab for analysis. Results are usually available within hours. The test is widely accessible and cost-effective, making it a first-line option in many hospitals. However, it’s critical to note that the test’s sensitivity is high, but its specificity is low. This means a positive result doesn’t confirm DVT—it only indicates the need for additional testing, such as ultrasound, to visualize the clot directly.
Age and medical history play a role in interpreting D-Dimer results. For instance, D-Dimer levels naturally increase with age, so cutoff values may be adjusted for older adults. Pregnant individuals, cancer patients, and those with chronic inflammatory conditions may also have elevated baseline levels, complicating interpretation. Clinicians must consider these factors to avoid false positives or negatives. Practical tips for patients include staying hydrated before the test, as dehydration can affect blood viscosity, and informing the healthcare provider of any recent illnesses or surgeries that might influence results.
In conclusion, the D-Dimer blood test is a valuable tool in the hospital’s arsenal for detecting DVT, but it’s not a standalone solution. Its ability to detect fibrin degradation makes it a sensitive initial screen, particularly in low-risk patients. However, positive results require follow-up imaging to confirm DVT. Understanding its limitations and contextualizing results based on patient-specific factors ensures accurate diagnosis and timely treatment, ultimately improving outcomes for those at risk.
Understanding the Role of an EVS Tech in Hospital Operations
You may want to see also
Explore related products






![]()
Venography: Injects contrast dye to highlight clots in vein X-rays
Venography stands as a definitive method for detecting deep vein thrombosis (DVT), offering unparalleled visualization of blood clots within deep veins. Unlike ultrasound, which relies on sound waves, venography employs X-ray technology combined with a contrast dye to create detailed images of the venous system. This procedure is particularly valuable in complex cases where other diagnostic tools may fall short, such as when clots are located in difficult-to-access areas or when there is a need for precise clot delineation.
The process begins with the injection of an iodine-based contrast dye into a vein, typically in the foot or ankle. The dye travels through the venous system, highlighting its structure on X-ray images. A series of X-rays, known as venograms, are then taken to capture the flow of the dye and identify any obstructions caused by clots. The contrast dye is both safe and effective, with dosages tailored to the patient’s age, weight, and kidney function to minimize risks. For instance, a standard adult dose ranges from 50 to 100 mL of contrast, while pediatric patients receive significantly lower amounts based on body surface area.
While venography is highly accurate, it is invasive and carries risks, including allergic reactions to the dye, infection, or bleeding at the injection site. Patients with severe kidney disease are particularly vulnerable, as the contrast dye can exacerbate renal function. Therefore, venography is reserved for cases where less invasive methods, such as compression ultrasound, are inconclusive or insufficient. It is also used when intervention, such as clot removal or stenting, is planned, as it provides real-time imaging to guide procedures.
Practical tips for patients undergoing venography include staying hydrated before and after the procedure to aid in dye excretion and informing the healthcare team of any allergies or kidney issues. The procedure itself takes approximately 30 to 60 minutes, with additional time for preparation and recovery. While discomfort is minimal, patients may experience a warm sensation as the dye is injected, and pressure at the injection site is common. Post-procedure, patients are monitored for adverse reactions and advised to resume normal activities unless otherwise instructed.
In comparison to other DVT detection methods, venography offers superior detail but at the cost of increased invasiveness and risk. Its role is complementary, serving as a confirmatory tool or a procedural guide rather than a first-line test. For clinicians, understanding when to employ venography—such as in suspected iliac vein thrombosis or when planning thrombolytic therapy—is critical. For patients, knowing what to expect can alleviate anxiety and ensure cooperation during the procedure. Ultimately, venography remains a cornerstone in the diagnostic and therapeutic management of DVT, particularly in challenging clinical scenarios.
Understanding Medicare Plan F: Hospital Stay Coverage Duration Explained
You may want to see also
Explore related products






![]()
Physical Examination: Checks for swelling, warmth, and redness in affected limbs
Swelling, warmth, and redness in a limb are telltale signs that prompt healthcare providers to suspect deep vein thrombosis (DVT). During a physical examination, the clinician will systematically assess these symptoms, comparing the affected limb to the unaffected one. Swelling, or edema, is often the most noticeable indicator, caused by blood pooling in the vein and leaking into surrounding tissues. Warmth in the area suggests inflammation, while redness may indicate increased blood flow or irritation. These findings, though nonspecific, are critical in guiding further diagnostic steps.
The process begins with a visual inspection, noting asymmetry between limbs. The clinician then palpates the area, assessing the degree of swelling and tenderness. A useful technique is the "pitting edema" test: applying pressure to the swollen area for a few seconds and observing whether an indentation remains. If it does, this confirms the presence of edema. Warmth is detected by gently touching the skin, comparing it to the unaffected limb or other areas of the body. Redness, often more pronounced in lighter skin tones, is evaluated under adequate lighting. These observations are documented in detail, as they provide a baseline for monitoring progression or resolution.
While physical examination is a cornerstone of DVT detection, it is not definitive. Swelling, warmth, and redness can also result from conditions like cellulitis, lymphedema, or muscle injury. For instance, cellulitis typically presents with more pronounced redness and pain, whereas lymphedema often involves chronic, non-pitting swelling. Therefore, clinicians must consider the patient’s medical history, risk factors (e.g., recent surgery, immobilization, or cancer), and other symptoms like pain or shortness of breath. This holistic approach ensures that DVT is neither missed nor misdiagnosed.
Practical tips for patients include monitoring symptoms at home, such as measuring the circumference of both limbs at the same location daily to track changes. Elevating the affected limb and avoiding tight clothing can reduce swelling and discomfort. However, self-assessment should never replace professional evaluation. If swelling, warmth, or redness develops suddenly or worsens, immediate medical attention is crucial. Early detection of DVT can prevent life-threatening complications like pulmonary embolism, making timely physical examination a vital tool in the diagnostic process.
Veterans Administration Hospital Nicknames: Unveiling the Unique Monikers
You may want to see also
Explore related products






![]()
Risk Factor Assessment: Evaluates medical history, surgery, immobility, and genetic predisposition
Hospitals begin DVT detection by scrutinizing risk factors, a critical step that transforms vague symptoms into actionable insights. Medical history takes center stage, with clinicians probing for prior DVT or pulmonary embolism episodes, as recurrence rates soar to 30% within a decade. Age emerges as a silent multiplier, with individuals over 60 facing a threefold increased risk due to vascular wall degradation. Chronic conditions like hypertension, diabetes, and heart disease further compound vulnerability, often necessitating tailored prophylaxis protocols during hospitalizations.
Surgical interventions act as acute risk accelerants, particularly in orthopedic and abdominal procedures. For instance, total hip replacement patients exhibit a 40-60% DVT incidence without prophylaxis, prompting routine administration of low-molecular-weight heparin (LMWH) at 40 mg daily for 10-14 days post-operation. Even minimally invasive surgeries aren’t exempt; laparoscopic cholecystectomy patients still warrant 5-7 days of LMWH or mechanical compression devices to mitigate immobilization-induced stasis.
Immobility, whether from surgery, trauma, or prolonged travel, disrupts venous flow dynamics, elevating DVT odds by 10-20%. Hospitals quantify this risk using tools like the Caprini score, assigning points for factors such as bedrest duration (e.g., 3 points for >72 hours) or active cancer (5 points). A cumulative score ≥3 typically triggers interventions like graduated compression stockings (GCS) with 15-30 mmHg pressure gradients, proven to reduce DVT risk by 50% in high-risk cohorts.
Genetic predisposition introduces an invisible yet potent risk layer, with Factor V Leiden mutation carriers facing a 5-10x higher DVT likelihood. Hospitals may order targeted tests like prothrombin gene mutation analysis for patients with unprovoked DVT or strong family histories. Positive results often necessitate extended anticoagulation therapy—up to 6-12 months with warfarin (INR 2.0-3.0) or direct oral anticoagulants (DOACs) like rivaroxaban 20 mg daily—to counteract lifelong hypercoagulability.
Integrating these risk factors into a structured assessment framework enables hospitals to stratify patients effectively. For instance, a 70-year-old post-knee replacement patient with Factor V Leiden would warrant aggressive prophylaxis: LMWH 40 mg daily, GCS, and early ambulation. Conversely, a young trauma patient with isolated lower extremity fracture might require only intermittent pneumatic compression. This precision approach not only optimizes resource allocation but also slashes DVT-related complications by up to 70% in high-risk populations.
Code Green: Hospital Emergency Response Protocol
You may want to see also
Frequently asked questions
DVT stands for Deep Vein Thrombosis, a condition where a blood clot forms in a deep vein, usually in the leg. Early detection is crucial as untreated DVT can lead to life-threatening complications like pulmonary embolism (PE).
Hospitals commonly use ultrasound (Doppler or duplex ultrasound) as the primary diagnostic tool to detect blood clots in deep veins. This non-invasive test provides clear images of blood flow and clot location.
Yes, if ultrasound is inconclusive, hospitals may use additional tests such as a D-dimer blood test (to check for clotting markers), CT venography, or MRI to confirm the diagnosis.
Common symptoms include swelling, pain, warmth, and redness in the affected limb. Hospitals also assess risk factors like recent surgery, prolonged immobility, or a history of clotting disorders.
With ultrasound, DVT can often be detected within hours of testing, allowing for prompt treatment to prevent complications. Early presentation to the hospital is key for timely diagnosis.