The number of rural hospitals in the United States is a critical aspect of the nation's healthcare infrastructure, particularly for communities in remote and underserved areas. As of recent data, there are approximately 1,800 rural hospitals across the country, serving as lifelines for millions of Americans who rely on them for essential medical care. However, these facilities face significant challenges, including financial strain, workforce shortages, and declining populations, which have led to a growing number of closures in recent years. Understanding the current landscape of rural hospitals is essential for addressing disparities in healthcare access and ensuring the well-being of rural populations.
| Characteristics | Values |
|---|---|
| Total Rural Hospitals (2023) | Approximately 1,800 |
| Percentage of All U.S. Hospitals | ~30% |
| Critical Access Hospitals (CAHs) | ~1,350 (as of 2023) |
| Rural Hospital Closures (2010-2023) | Over 130 |
| States with Most Rural Hospitals | Texas, Kansas, and Missouri |
| Average Bed Size | 25-50 beds (varies by hospital type) |
| Financial Challenges | ~40% operate at a loss; ~20% at risk of closure (as of 2023) |
| Population Served | ~20% of the U.S. population lives in rural areas |
| Healthcare Workforce Shortages | Significant shortages in physicians, nurses, and specialists |
| COVID-19 Impact | Accelerated financial strain and closures |
| Policy Support | Programs like Medicare Rural Hospital Flexibility Program, CAH designation |
Explore related products






What You'll Learn
![]()
Total rural hospitals in the U.S
As of recent data, the United States is home to approximately 1,800 rural hospitals, a figure that underscores the critical role these institutions play in providing healthcare access to millions of Americans living outside urban centers. These hospitals are often the sole providers of medical services in their communities, offering emergency care, primary care, and specialized treatments that would otherwise be inaccessible. Despite their importance, rural hospitals face unique challenges, including financial instability, workforce shortages, and aging infrastructure, which threaten their long-term viability.
Analyzing the distribution of these hospitals reveals a stark disparity across regions. The South, for instance, hosts the largest number of rural hospitals, reflecting both the region’s vast rural population and its higher rates of chronic health conditions. In contrast, the Northeast has fewer rural hospitals, partly due to its smaller rural population and greater proximity to urban healthcare hubs. This regional variation highlights the need for tailored policies to address the specific challenges faced by rural hospitals in different parts of the country.
From a financial perspective, rural hospitals operate on thin margins, with many relying heavily on Medicare and Medicaid reimbursements. These reimbursements often fall short of covering the cost of care, particularly for hospitals serving low-income populations. To survive, many rural hospitals have adopted innovative strategies, such as telemedicine programs, partnerships with larger health systems, and diversification of services to include outpatient care and preventive health initiatives. These efforts are essential for ensuring the sustainability of rural healthcare.
A comparative look at rural hospitals versus their urban counterparts reveals significant differences in resources and patient demographics. Rural hospitals typically have fewer beds, limited specialty services, and higher proportions of elderly patients. They also face greater challenges in recruiting and retaining healthcare professionals, often relying on traveling nurses and physicians to fill gaps. Despite these limitations, rural hospitals achieve comparable patient outcomes in many areas, a testament to the dedication of their staff and the resilience of their communities.
For policymakers and healthcare advocates, understanding the total number of rural hospitals is just the starting point. The real challenge lies in addressing the systemic issues that imperil their existence. This includes advocating for increased federal funding, expanding loan forgiveness programs for rural healthcare workers, and investing in technology to bridge the urban-rural healthcare divide. By taking these steps, we can ensure that rural hospitals continue to serve as lifelines for the communities that depend on them.
Mercy Hospital: Pain Clinic Availability and Services
You may want to see also
Explore related products






![]()
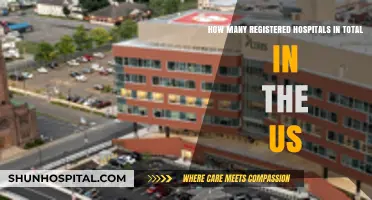
Rural hospital closures by state
Rural hospital closures have disproportionately affected certain states, creating a patchwork of healthcare access across the U.S. Texas leads the nation with the highest number of rural hospital closures since 2010, totaling 27 as of 2023. This trend is partly due to the state’s refusal to expand Medicaid under the Affordable Care Act, leaving many rural hospitals without critical reimbursement funds. Tennessee follows closely, with 20 closures, while Oklahoma has seen 14 hospitals shut their doors. These states share common challenges: aging populations, low reimbursement rates, and a heavy reliance on federal funding that often falls short of operational costs.
Analyzing the data reveals a stark divide between states that have expanded Medicaid and those that haven’t. States like Kentucky and Arkansas, which expanded Medicaid, have experienced fewer closures compared to their non-expansion counterparts. For instance, Kentucky has only seen 5 closures, while neighboring Tennessee, a non-expansion state, has faced quadruple that number. This suggests that Medicaid expansion provides a financial lifeline to rural hospitals by increasing insured patient volumes and reducing uncompensated care costs. Policymakers in states with high closure rates could consider this as a strategic intervention to stabilize rural healthcare systems.
The impact of closures extends beyond healthcare, rippling through local economies. In Alabama, where 16 rural hospitals have closed, communities have lost not only emergency services but also major employers. A single rural hospital closure can result in the loss of 100 to 150 jobs, exacerbating economic decline in already struggling areas. To mitigate this, some states, like Georgia, have implemented rural hospital tax credits and loan forgiveness programs for healthcare professionals willing to work in underserved areas. These initiatives, while not a panacea, offer a model for addressing both healthcare and economic challenges simultaneously.
Comparing closure rates by region highlights the role of geography in healthcare disparities. The Southeast and Midwest have been hit hardest, with states like Mississippi and Kansas reporting 12 and 11 closures, respectively. These regions often have higher poverty rates and fewer alternative healthcare providers, making closures particularly devastating. In contrast, states in the Northeast, such as Maine and Vermont, have seen fewer closures, partly due to denser populations and stronger state-level healthcare investments. This regional disparity underscores the need for tailored solutions that account for local demographics and infrastructure.
To address rural hospital closures effectively, states must adopt multi-faceted strategies. First, expanding Medicaid in non-expansion states could provide immediate financial relief. Second, investing in telehealth infrastructure can bridge gaps in access, though this requires broadband expansion in rural areas. Third, incentivizing healthcare professionals to practice in rural areas through loan repayment programs and competitive salaries can help sustain existing facilities. Finally, state and federal policymakers should collaborate to create flexible funding models that account for the unique challenges of rural healthcare. Without such interventions, the trend of closures will continue, leaving millions of Americans without critical care.
Safe Hospital Waste Disposal: Best Practices
You may want to see also
Explore related products






![]()
Critical Access Hospitals (CAHs) count
As of recent data, the United States has approximately 1,350 rural hospitals, a number that has been steadily declining due to financial pressures, population shifts, and operational challenges. Among these, Critical Access Hospitals (CAHs) represent a significant subset, specifically designed to address the unique needs of rural communities. Established by the Balanced Budget Act of 1997, CAHs are limited to 25 beds and must provide 24/7 emergency care, ensuring rural residents have access to essential healthcare services. Understanding the CAH count is crucial, as these facilities are often the only healthcare providers in their regions, serving as lifelines for millions of Americans.
To qualify as a CAH, a hospital must meet specific criteria, including being located more than 35 miles from another hospital or 15 miles in areas with mountainous terrain. As of 2023, there are over 1,300 CAHs across the U.S., accounting for nearly all rural hospitals. This designation provides financial benefits, such as cost-based reimbursement from Medicare, which helps sustain operations in low-population areas. However, the CAH program is not without challenges; these hospitals often struggle with workforce shortages, outdated infrastructure, and limited resources, making their survival critical yet precarious.
Analyzing the CAH count reveals regional disparities. States like Texas, Kansas, and Nebraska have the highest number of CAHs, reflecting their vast rural landscapes. Conversely, states with denser populations, such as New Jersey and Connecticut, have fewer CAHs. This distribution highlights the program’s effectiveness in targeting areas with the greatest need but also underscores the vulnerability of rural healthcare systems. For instance, the closure of a single CAH in a remote area can leave residents with no nearby emergency care, forcing them to travel long distances for treatment.
For policymakers and healthcare advocates, the CAH count serves as a barometer of rural healthcare accessibility. Efforts to support these hospitals include increasing Medicare reimbursements, expanding telehealth services, and providing grants for facility upgrades. Practical tips for communities include advocating for local CAHs, participating in health fairs, and supporting initiatives that address workforce shortages, such as loan forgiveness programs for rural healthcare providers. By focusing on the CAH count and its implications, stakeholders can work toward preserving this vital component of the U.S. healthcare system.
In conclusion, the CAH count is more than just a statistic—it represents the resilience and challenges of rural healthcare in America. With over 1,300 CAHs serving as critical access points for care, their role cannot be overstated. Yet, their sustainability depends on continued support, innovative solutions, and a commitment to addressing the unique needs of rural populations. As rural hospitals face an uncertain future, the CAH program remains a cornerstone of efforts to ensure equitable healthcare access nationwide.
The Hospital's Leader: Who's in Charge?
You may want to see also
Explore related products






![]()
Rural vs. urban hospital distribution
The United States is home to approximately 1,800 rural hospitals, a figure that highlights both their critical role in healthcare access and their precarious financial existence. These facilities serve as lifelines for nearly 50 million Americans living in rural areas, providing essential services from emergency care to chronic disease management. Despite their importance, rural hospitals face unique challenges, including lower patient volumes, higher operating costs, and limited reimbursement rates, which have led to over 130 closures since 2010. This contrasts sharply with urban hospitals, which number around 3,000 and benefit from denser populations, higher revenue streams, and greater access to specialized resources.
Analyzing the distribution of hospitals reveals a stark disparity in healthcare infrastructure. Urban areas, with their concentrated populations, often have multiple hospitals within a short radius, offering specialized care and advanced technologies. For instance, metropolitan regions like New York City or Los Angeles boast dozens of hospitals, many affiliated with prestigious medical schools or research institutions. In contrast, rural areas frequently have just one hospital serving an entire county or region, often with limited capacity and fewer specialists. This imbalance exacerbates health inequities, as rural residents may face longer travel times for critical care, delayed treatments, and reduced access to preventive services.
To address this gap, policymakers and healthcare leaders must prioritize strategies tailored to rural needs. One effective approach is expanding telehealth services, which can bridge the distance barrier by connecting rural patients with urban specialists. For example, remote consultations for conditions like diabetes or mental health can improve outcomes without requiring patients to travel. Additionally, financial incentives such as increased Medicare reimbursements or grants for rural hospitals can stabilize their operations. States like Texas and North Carolina have implemented rural hospital flexibility programs, allowing facilities to repurpose unused beds for community health needs, thereby enhancing sustainability.
A comparative analysis of rural and urban hospital staffing further underscores the divide. Urban hospitals typically employ a diverse workforce, including subspecialists, researchers, and administrative staff, supported by robust budgets. Rural hospitals, on the other hand, often rely on general practitioners, nurse practitioners, and traveling healthcare professionals to fill gaps. This staffing disparity affects the scope of services offered; rural hospitals may struggle to provide advanced care like oncology or neurology, forcing patients to seek treatment elsewhere. Investing in rural healthcare education programs, such as loan forgiveness for providers who commit to rural practice, could help alleviate this shortage.
Ultimately, the rural vs. urban hospital distribution issue is not just about numbers but about equity and accessibility. While urban hospitals thrive in environments of abundance, rural hospitals operate in a landscape of scarcity, requiring innovative solutions to survive and serve their communities. By focusing on policy reforms, technological integration, and workforce development, stakeholders can ensure that rural hospitals remain viable, narrowing the healthcare divide and improving outcomes for millions of Americans.
LOA Days: Impacting Hospital Statistics and Performance
You may want to see also
Explore related products




$9.09 $10.99


![]()
Trends in rural hospital numbers
The number of rural hospitals in the U.S. has been steadily declining over the past two decades, with over 130 closures since 2010. This trend is particularly alarming given that rural hospitals serve as critical lifelines for approximately 46 million Americans. Financial pressures, including low patient volumes, high operating costs, and reduced reimbursement rates from Medicare and Medicaid, are primary drivers of these closures. Smaller hospitals often struggle to maintain profitability, especially in areas with aging populations and limited economic opportunities. As a result, rural communities face increasing challenges in accessing essential healthcare services, exacerbating existing health disparities.
One notable trend is the shift toward alternative healthcare delivery models in rural areas. Telehealth, for instance, has emerged as a viable solution to bridge the gap created by hospital closures. During the COVID-19 pandemic, telehealth usage in rural areas increased by 154%, demonstrating its potential to improve access to care. However, this approach is not without limitations; reliable broadband access remains a significant barrier in many rural communities. Additionally, some services, such as emergency care and surgical procedures, cannot be fully replaced by virtual solutions. Policymakers and healthcare providers must address these challenges to ensure telehealth complements, rather than replaces, traditional care models.
Another trend is the consolidation of rural hospitals into larger health systems. Mergers and acquisitions have become increasingly common as smaller facilities seek financial stability and operational support. While consolidation can improve efficiency and resource sharing, it often leads to reduced local autonomy and potential service cuts. For example, a merged hospital might prioritize profitable services over those critical to the community, such as obstetrics or mental health care. Rural residents must advocate for their needs during these transitions to prevent further erosion of healthcare access.
Despite these challenges, innovative strategies are emerging to sustain rural hospitals. Critical Access Hospitals (CAHs), which account for nearly 40% of rural hospitals, benefit from enhanced Medicare reimbursements and operational flexibility. However, CAHs must meet specific criteria, including a limit of 25 acute care beds and an average length of stay under 96 hours. Additionally, state and federal initiatives, such as the Rural Emergency Hospital designation, offer financial incentives for facilities to reconfigure their services. These models demonstrate that with targeted support, rural hospitals can adapt to changing demands and remain viable.
In conclusion, the decline in rural hospital numbers reflects broader systemic issues in U.S. healthcare. While closures continue to threaten access, trends like telehealth expansion, consolidation, and innovative designations offer pathways forward. Addressing these challenges requires a multifaceted approach, combining policy interventions, technological advancements, and community engagement. Without concerted effort, the loss of rural hospitals will deepen health inequities and leave millions of Americans without critical care.
VA Hospital: Offering a Barber Shop Service?
You may want to see also
Frequently asked questions
As of 2023, there are approximately 1,800 rural hospitals in the United States, though this number fluctuates due to closures and openings.
Rural hospitals make up about 30-35% of all hospitals in the US, depending on the classification criteria used.
Over 130 rural hospitals have closed since 2010, with the majority of closures occurring in the past decade due to financial challenges.
States like Texas, Georgia, and Kansas have some of the highest numbers of rural hospitals due to their large rural populations and geographic size.
A rural hospital is typically defined as a facility located outside of urban areas, often serving populations in remote or sparsely populated regions, as classified by the Centers for Medicare & Medicaid Services (CMS) or the Office of Management and Budget (OMB).