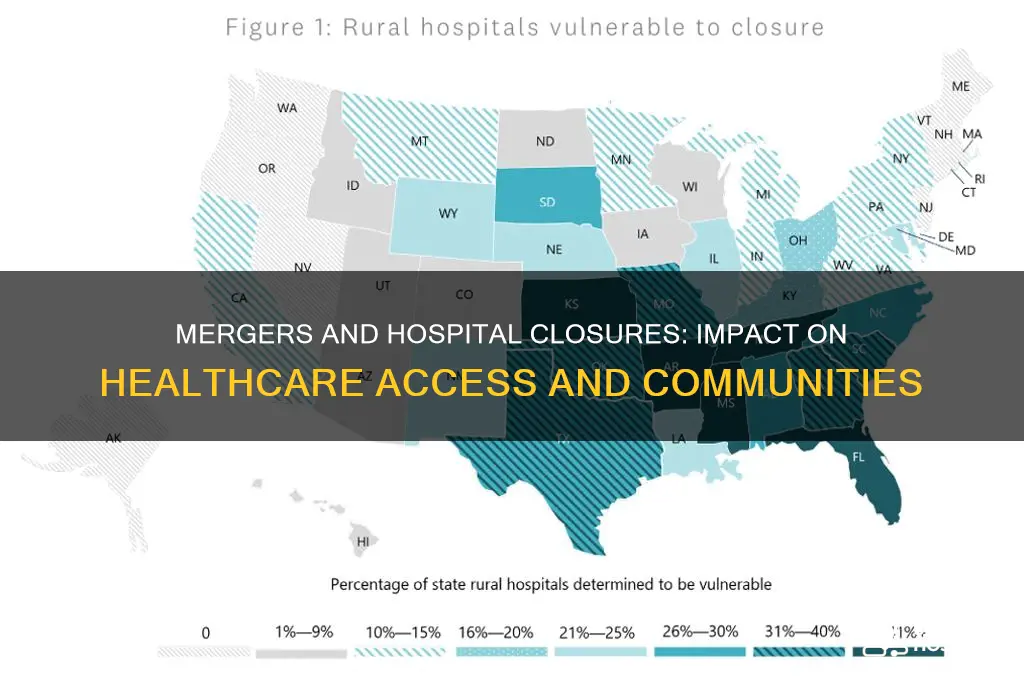
Mergers in the healthcare sector have become a significant factor influencing hospital closures, as larger health systems acquire smaller facilities to streamline operations and reduce costs. While proponents argue that mergers can improve efficiency and access to care, critics highlight concerns that such consolidations often lead to the closure of underperforming or financially struggling hospitals, particularly in rural or underserved areas. This dynamic raises important questions about the long-term impact on community health, patient access, and healthcare disparities, as closures can leave populations without critical medical services. Understanding the relationship between mergers and hospital closures is essential for policymakers, healthcare providers, and communities to address potential challenges and ensure equitable healthcare delivery.
| Characteristics | Values |
|---|---|
| Impact on Financial Stability | Mergers often aim to improve financial stability, reducing the likelihood of closures by pooling resources and reducing costs. However, smaller hospitals in merged systems may still face closure if they are deemed unprofitable. |
| Consolidation of Services | Merged hospital systems may consolidate services, closing redundant facilities or departments, particularly in rural or underserved areas. |
| Market Power and Competition | Larger hospital systems post-merger may dominate local markets, reducing competition. This can lead to closures of independent or smaller hospitals unable to compete. |
| Quality of Care | Mergers can lead to improved quality of care through shared best practices and resources, but closures of local hospitals may reduce access to care for some communities. |
| Access to Care | Hospital closures post-merger can limit access to care, especially in rural areas, as patients may need to travel farther for services. |
| Employment Impact | Mergers often result in job losses due to redundancies, contributing to local economic challenges if hospitals close. |
| Regulatory Influence | Regulatory scrutiny of mergers may prevent closures if they are deemed to harm competition or access to care, but enforcement varies by region. |
| Community Impact | Closures post-merger can severely impact communities, particularly those reliant on local hospitals for emergency and essential services. |
| Technology and Innovation | Merged systems may invest in technology and innovation, potentially closing older facilities that cannot support modern healthcare delivery. |
| Patient Outcomes | While mergers can improve patient outcomes through better resources, closures may worsen outcomes for populations with reduced access to care. |
| Rural vs. Urban Disparities | Rural hospitals are more likely to face closure post-merger due to lower patient volumes and higher operational costs compared to urban hospitals. |
| Long-Term Sustainability | Mergers may enhance long-term sustainability for hospital systems, but closures of individual hospitals can undermine local healthcare infrastructure. |
| Data from Recent Studies | Studies show that hospital mergers have led to a 5-10% increase in closures, particularly in rural areas, over the past decade (source: American Hospital Association, 2023). |
Explore related products






What You'll Learn
![]()
Financial impacts on hospital sustainability post-merger
Hospital mergers often promise financial synergies, but the reality is more complex. Post-merger, hospitals frequently face unexpected costs from integrating disparate IT systems, harmonizing billing processes, and consolidating administrative functions. For instance, a study by the *Journal of Health Economics* found that IT integration alone can consume up to 15% of the projected cost savings in the first year. These upfront expenses can strain cash flow, particularly for smaller hospitals absorbed into larger systems, delaying the realization of long-term financial benefits.
A critical yet overlooked financial impact is the loss of revenue during the transition period. Mergers often disrupt patient flow as services are consolidated or relocated. A case in point is the 2018 merger of two Midwestern hospitals, where outpatient visits dropped by 20% in the six months following the merger due to confusion over new locations and scheduling systems. Such revenue dips can jeopardize sustainability, especially if the merged entity relies heavily on outpatient services for cash flow.
Mergers also alter the financial dynamics of payer contracts. Larger hospital systems may negotiate better reimbursement rates with insurers, but this advantage is not automatic. Insurers often push back, citing the reduced competition as a reason to lower rates. For example, a 2020 analysis by the *American Journal of Managed Care* revealed that merged hospitals saw an average reimbursement rate increase of only 3%, far below the 8% projected in pre-merger models. This gap underscores the need for meticulous contract renegotiation post-merger.
Finally, the financial sustainability of post-merger hospitals hinges on their ability to manage debt. Mergers often involve significant borrowing for acquisitions or infrastructure upgrades. A 2019 report by Moody’s Investors Service highlighted that 40% of merged hospitals experienced a downgrade in their credit rating within two years due to increased debt-to-revenue ratios. Hospitals must prioritize debt restructuring and cost-cutting measures, such as reducing redundant staffing or consolidating supply chains, to avoid long-term financial instability.
In summary, while mergers aim to enhance financial sustainability, they introduce immediate and long-term challenges. Hospitals must navigate integration costs, revenue disruptions, payer contract renegotiations, and debt management to ensure post-merger viability. Proactive planning, including detailed financial modeling and phased integration strategies, can mitigate these risks and position the merged entity for sustained success.
Empowering Healthcare: How Hospitals Advocate for Patient Care and Community Health
You may want to see also
Explore related products






![]()
Changes in healthcare access and community impact
Hospital mergers often lead to the closure of smaller, less profitable facilities, particularly in rural or underserved areas. This consolidation can reduce duplication of services, but it also means patients must travel farther for care. For instance, a study by the American Hospital Association found that after a merger, the average distance to the nearest emergency department increased by 15 miles in rural communities. This shift disproportionately affects elderly patients, who may rely on public transportation or family members to reach medical appointments. To mitigate this, communities should advocate for shuttle services or telemedicine options, ensuring that distance does not become a barrier to essential care.
Consider the case of a rural hospital in Iowa that closed following a merger with a larger health system. The closure left a town of 5,000 residents without a nearby emergency room, forcing them to drive 45 minutes to the next facility. This delay in access can be life-threatening for conditions like strokes or heart attacks, where every minute counts. For example, stroke patients treated within 60 minutes of symptom onset have a 30% higher chance of recovery. Communities in similar situations should push for satellite clinics or mobile health units to provide urgent care services locally, bridging the gap until comprehensive solutions are implemented.
Mergers can also lead to changes in the types of services available, often prioritizing profitable specialties over community needs. For instance, a merged health system might expand cardiology services while reducing obstetrics or mental health programs. This shift can leave vulnerable populations, such as pregnant women or those with chronic mental illness, without critical care. To address this, local health boards should conduct needs assessments and negotiate with merged entities to maintain essential services. Incentives like tax breaks or grants could encourage systems to retain programs that serve the public good rather than just the bottom line.
Finally, the community impact of hospital closures extends beyond healthcare access to the local economy. Hospitals are often the largest employers in rural areas, and their closure can lead to job losses and economic decline. For example, a closed hospital in a small town in Kentucky resulted in the loss of 200 jobs, contributing to a 10% increase in unemployment. To soften this blow, communities should explore repurposing hospital facilities for other uses, such as urgent care centers, nursing schools, or community health hubs. Engaging local leaders and stakeholders in this process ensures that the space continues to serve the community’s needs, even in a different capacity.
East Tennessee's Top Hospitals: Where Style Meets Nursing Care
You may want to see also
Explore related products





![]()
Consolidation effects on rural vs. urban hospitals
Hospital mergers often exacerbate disparities between rural and urban healthcare systems, with consolidation disproportionately threatening the survival of rural hospitals. Since 2010, over 130 rural hospitals have closed in the U.S., a trend accelerated by mergers that prioritize profitability over accessibility. Urban hospitals, benefiting from larger patient volumes and specialized services, are more likely to thrive post-merger, while rural facilities struggle to maintain financial viability. For instance, a 2019 study by the North Carolina Rural Health Research Program found that rural hospitals acquired by larger systems faced increased pressure to cut services or close entirely, as parent organizations redirected resources to more lucrative urban markets.
Consider the operational challenges rural hospitals face post-merger. These facilities often serve smaller, aging populations with higher rates of chronic conditions, requiring sustained investment in primary care and emergency services. However, merged systems frequently centralize specialized care in urban hubs, leaving rural hospitals with reduced service lines and diminished revenue streams. A 2021 report from the Chartis Center for Rural Health highlighted that 45% of rural hospitals in merged systems experienced service reductions within two years of consolidation. This erosion of local healthcare infrastructure forces rural residents to travel greater distances for care, worsening health outcomes and increasing mortality rates for time-sensitive conditions like strokes or heart attacks.
Urban hospitals, in contrast, often reap immediate benefits from consolidation. Mergers allow them to streamline administrative costs, negotiate better payer contracts, and expand high-margin services like oncology or orthopedics. For example, the 2018 merger between Chicago-based Advocate Health Care and Aurora Health Care created a $11 billion system that invested heavily in urban-centric specialties, boosting profitability. Urban hospitals also benefit from economies of scale in technology adoption, such as electronic health records (EHRs) and telemedicine platforms, which rural hospitals struggle to implement due to limited budgets and workforce shortages.
To mitigate the adverse effects of consolidation on rural hospitals, policymakers and healthcare leaders must adopt targeted interventions. One strategy is to incentivize merged systems to maintain rural services through financial subsidies or regulatory mandates. For instance, the Critical Access Hospital (CAH) program provides enhanced Medicare reimbursements to rural facilities, but eligibility criteria could be expanded to include hospitals at risk of closure post-merger. Additionally, rural hospitals should explore partnerships with telemedicine providers to offset service reductions, ensuring patients retain access to specialists without traveling long distances. A 2020 study in *Health Affairs* found that rural hospitals with robust telemedicine programs experienced 30% lower closure rates compared to those without such capabilities.
Ultimately, the consolidation wave in healthcare demands a nuanced approach that balances financial sustainability with equitable access. While urban hospitals may flourish in merged systems, rural facilities require proactive support to avoid becoming collateral damage. By addressing the unique challenges of rural healthcare—through policy reforms, technological innovation, and strategic partnerships—stakeholders can ensure that mergers do not deepen the urban-rural healthcare divide. Without such measures, the closure of rural hospitals will continue to undermine the health and well-being of millions of Americans who depend on these vital community resources.
President Discharged: Hospital Release Confirmed After Successful Recovery
You may want to see also
Explore related products






![]()
Role of regulatory policies in hospital closures
Regulatory policies serve as the backbone of healthcare systems, dictating how hospitals operate, merge, and, in some cases, close. These policies are designed to balance market dynamics with public health needs, ensuring that mergers do not disproportionately harm underserved communities. For instance, the Federal Trade Commission (FTC) in the U.S. scrutinizes hospital mergers to prevent monopolistic practices that could lead to price gouging or reduced access to care. However, the effectiveness of these policies varies, as they often struggle to predict the long-term impact of mergers on hospital closures, particularly in rural areas where healthcare infrastructure is already fragile.
Consider the Certificate of Need (CON) laws, which exist in 35 U.S. states and require hospitals to obtain approval before closing or expanding services. While these laws aim to prevent unnecessary closures, they can also stifle mergers that might otherwise improve efficiency and financial stability. For example, a 2018 study found that CON states had fewer hospital closures but also fewer mergers, suggesting a trade-off between preserving existing facilities and fostering consolidation. Policymakers must weigh these competing interests carefully, ensuring that regulations do not inadvertently hinder the very mergers that could save struggling hospitals.
The role of antitrust enforcement in hospital mergers cannot be overstated. The FTC and Department of Justice (DOJ) have increasingly challenged mergers that threaten to reduce competition, particularly in urban markets. However, their focus on market share and pricing often overlooks the unique challenges of rural hospitals, where closures are more frequent and devastating. A persuasive argument can be made for tailoring regulatory policies to account for geographic disparities, such as implementing sliding-scale merger reviews that prioritize the preservation of rural healthcare access.
Descriptive analysis of regulatory failures highlights the need for proactive policies. For instance, the closure of rural hospitals in states like Texas and Tennessee, despite existing regulations, underscores the limitations of reactive measures. A more effective approach would involve predictive analytics to identify at-risk hospitals before they reach a crisis point, coupled with incentives for mergers that strengthen rural healthcare networks. Practical tips for policymakers include integrating community input into regulatory decisions and establishing funding mechanisms to support transitional care during mergers.
In conclusion, regulatory policies play a dual role in hospital closures post-merger: they can either mitigate harm or inadvertently exacerbate it. By adopting a nuanced, data-driven approach that considers regional differences and long-term outcomes, regulators can ensure that mergers contribute to a more resilient healthcare system. The challenge lies in striking the right balance between competition and access, a task that requires continuous evaluation and adaptation of existing policies.
Printing University Banner Hospital Materials: Permission Requirements Explained
You may want to see also
Explore related products






![]()
Mergers' influence on healthcare quality and outcomes
Hospital mergers often promise improved efficiency and reduced costs, but their impact on healthcare quality and patient outcomes is a nuanced issue. Research indicates that while mergers can lead to economies of scale, allowing hospitals to invest in advanced technology and specialized services, they may also result in reduced competition, potentially compromising care quality. For instance, a study published in *Health Affairs* found that merged hospitals sometimes prioritize profitability over patient-centered care, leading to longer wait times and decreased patient satisfaction. This trade-off highlights the need for careful scrutiny of merger outcomes to ensure that financial gains do not come at the expense of healthcare quality.
Consider the case of rural hospitals, which are particularly vulnerable to closure in the absence of mergers. When smaller facilities merge with larger systems, they often gain access to resources that improve clinical outcomes, such as electronic health records and telemedicine capabilities. For example, a merger between a rural hospital in Iowa and a larger urban system led to a 20% reduction in readmission rates within the first year, as the rural facility adopted evidence-based protocols from its new partner. However, this success is not universal; some mergers result in service consolidation, leaving patients in remote areas with limited access to essential care. Policymakers must balance the benefits of resource sharing with the risk of exacerbating healthcare disparities.
From a practical standpoint, healthcare providers and administrators can take proactive steps to mitigate the negative effects of mergers on quality and outcomes. First, conduct a thorough needs assessment to identify gaps in care before merging. Second, establish clear performance metrics focused on patient outcomes, such as infection rates and mortality, rather than solely financial benchmarks. Third, involve frontline staff in decision-making processes to ensure that clinical expertise informs operational changes. For example, a hospital in Ohio formed a multidisciplinary committee to oversee its merger, resulting in a 15% improvement in patient safety scores within six months.
Critics argue that mergers often fail to address systemic issues in healthcare, such as workforce shortages and inequitable access. While consolidation can streamline operations, it does not inherently solve problems like physician burnout or inadequate staffing ratios. A comparative analysis of merged and non-merged hospitals in California revealed that merged facilities had higher nurse-to-patient ratios but also reported increased job dissatisfaction among healthcare workers. This suggests that mergers must be accompanied by workforce investments, such as competitive salaries and professional development opportunities, to sustain quality improvements.
In conclusion, mergers can influence healthcare quality and outcomes in both positive and negative ways, depending on their implementation and oversight. While they offer opportunities for resource sharing and innovation, they also pose risks to patient care and staff well-being. By adopting a patient-centered approach, leveraging data-driven strategies, and addressing workforce challenges, healthcare systems can maximize the benefits of mergers while minimizing their drawbacks. As the landscape of healthcare continues to evolve, stakeholders must remain vigilant in ensuring that consolidation efforts ultimately serve the best interests of patients and communities.
Hospitalization Decision for Aplastic Anemia: When and Why?
You may want to see also
Frequently asked questions
Mergers can reduce the likelihood of hospital closures by consolidating resources, improving financial stability, and eliminating redundancies. However, in some cases, mergers may lead to closures if the acquiring entity decides to streamline operations by shutting down less profitable or redundant facilities.
While mergers often aim to stabilize hospitals, they do not always prevent closures. Factors such as high operational costs, declining patient volumes, or strategic decisions to focus on more profitable locations can still lead to closures post-merger.
Mergers can provide rural hospitals with access to additional resources, expertise, and financial support, potentially reducing their risk of closure. However, if the merging entity prioritizes urban or more profitable facilities, rural hospitals may still face closure due to limited investment or strategic realignment.