Reducing hospital readmission rates is a critical focus in healthcare, as it not only improves patient outcomes but also enhances cost-efficiency and resource utilization. A nursing project aimed at addressing this issue requires a systematic approach, beginning with identifying the root causes of readmissions, such as inadequate patient education, lack of follow-up care, or poor discharge planning. Nurses play a pivotal role in this process by implementing evidence-based interventions, such as comprehensive discharge teaching, medication reconciliation, and coordinating post-discharge support services. The project should also incorporate data analysis to track readmission trends and measure the effectiveness of interventions. Collaboration with interdisciplinary teams, patient engagement, and continuous evaluation are essential to ensure sustainable improvements in reducing readmission rates and fostering better long-term health for patients.
Explore related products






What You'll Learn
- Identify high-risk patients using data analysis and predictive modeling to target interventions effectively
- Enhance discharge planning by providing clear instructions, medication reconciliation, and follow-up appointments
- Improve patient education on self-care, symptom management, and when to seek medical attention post-discharge
- Strengthen post-discharge support through home health services, telehealth, and community resource referrals
- Evaluate and refine protocols by tracking readmission data and adjusting strategies based on outcomes
![]()
Identify high-risk patients using data analysis and predictive modeling to target interventions effectively
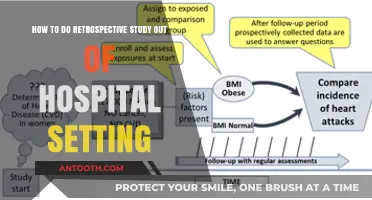
Hospital readmissions strain healthcare systems and often indicate gaps in patient care. Identifying high-risk patients before discharge is crucial for targeted interventions. Data analysis and predictive modeling offer powerful tools to achieve this, moving beyond intuition and general risk factors.
By leveraging electronic health records (EHRs), claims data, and social determinants of health, nurses can pinpoint patients most likely to return to the hospital.
Consider a patient with congestive heart failure, a condition notorious for high readmission rates. Predictive models can analyze factors like age (over 65), medication adherence (less than 80% compliance), recent hospitalizations (two or more in the past six months), and socioeconomic status (low income, lack of social support). These variables, when fed into algorithms, generate a risk score. Patients scoring above a certain threshold are flagged for intensive discharge planning, which might include:
- Structured medication reconciliation: Ensuring patients understand their medications, dosages (e.g., 20mg lisinopril daily), and potential side effects.
- Telehealth follow-up appointments: Scheduling virtual check-ins within 72 hours of discharge to monitor symptoms and address concerns promptly.
- Connection to community resources: Referring patients to local food banks, transportation services, or home health aides to address social determinants impacting health.
While data-driven risk stratification is promising, ethical considerations are paramount. Transparency in model development and use is essential, ensuring patients understand how their data is being utilized. Additionally, models must be regularly audited for bias and fairness, preventing discrimination against vulnerable populations.
It's crucial to remember that predictive models are tools, not crystal balls. They provide probabilities, not certainties. Nurses must use their clinical judgment and patient interaction to refine risk assessments and tailor interventions accordingly.
By integrating data analysis and predictive modeling into nursing practice, we can move from reactive to proactive care, ultimately reducing hospital readmissions and improving patient outcomes. This approach empowers nurses to become data-informed advocates, ensuring that limited resources are directed to those who need them most.
Praying for Hospitalized Loved Ones: A Guide to Compassionate Intercession
You may want to see also
Explore related products






![]()
Enhance discharge planning by providing clear instructions, medication reconciliation, and follow-up appointments
Effective discharge planning is a critical intervention to reduce hospital readmission rates, yet it often falls short due to gaps in communication and coordination. Patients, particularly older adults or those with chronic conditions, frequently leave the hospital without a clear understanding of their post-discharge care plan. For instance, a study published in the *Journal of the American Medical Association* found that nearly 20% of Medicare beneficiaries are readmitted within 30 days, often due to medication errors or lack of follow-up care. To address this, nurses must prioritize three key components: clear instructions, medication reconciliation, and scheduling follow-up appointments. These steps not only empower patients but also ensure continuity of care, reducing the likelihood of complications that lead to readmission.
Clear instructions are the cornerstone of successful discharge planning. Patients should receive written and verbal guidance tailored to their health literacy level. For example, instead of generic phrases like "take as directed," specify exact dosages, such as "take 500 mg of metformin twice daily with meals." Visual aids, like medication schedules or diagrams, can further enhance understanding. Nurses should also address potential side effects and red flags, such as "call your doctor immediately if you experience shortness of breath or swelling in your legs." For patients with limited English proficiency or cognitive impairments, involve translators or caregivers to ensure comprehension. Practical tips, such as using pill organizers or setting medication reminders, can also improve adherence and reduce confusion.
Medication reconciliation is another vital step often overlooked during discharge. Discrepancies in medication lists—such as omitted prescriptions, incorrect dosages, or drug interactions—account for a significant portion of readmissions. Nurses should conduct a thorough review of the patient’s pre-admission, in-hospital, and discharge medications, reconciling any differences. For example, if a patient was taking lisinopril 10 mg at home but received 20 mg in the hospital, clarify whether the dosage change is intentional and document it. Tools like electronic health records (EHRs) with built-in reconciliation features can streamline this process. Additionally, pharmacists can be consulted to identify potential interactions, such as combining warfarin with antibiotics that increase bleeding risk.
Scheduling follow-up appointments before discharge is the final piece of the puzzle. Delayed or missed appointments disrupt care continuity and increase readmission risk. Nurses should coordinate with primary care providers or specialists to secure appointments within 7–14 days of discharge, particularly for high-risk patients like those with heart failure or diabetes. For example, a patient discharged after a heart attack should have a cardiology follow-up scheduled to monitor ejection fraction and adjust medications like beta-blockers or ACE inhibitors. Transportation barriers should also be addressed; offering resources like medical transport services or telehealth options can improve attendance. A well-documented discharge summary, including lab results and pending tests, ensures providers have the necessary information to continue care seamlessly.
By integrating clear instructions, medication reconciliation, and follow-up appointments into discharge planning, nurses can significantly reduce readmission rates. These steps not only improve patient outcomes but also foster trust and confidence in the healthcare system. For instance, a study in *The New England Journal of Medicine* demonstrated that structured discharge interventions reduced readmissions by 25% in high-risk populations. However, success requires collaboration across disciplines and a commitment to patient-centered care. Nurses must advocate for resources like extended discharge times, access to translators, and EHR tools to support these efforts. Ultimately, enhancing discharge planning is not just a task—it’s a transformative strategy to improve care quality and reduce hospital readmissions.
Is Dr. Eldred Wiser Related to the Wiser Hospital Doctor?
You may want to see also
Explore related products






![]()
Improve patient education on self-care, symptom management, and when to seek medical attention post-discharge
Effective patient education is a cornerstone of reducing hospital readmissions, yet it remains an underutilized strategy. Many patients leave the hospital with a vague understanding of their condition, medications, and warning signs, leading to complications that could have been avoided. For instance, a study published in the *Journal of Nursing Care Quality* found that patients who received structured discharge education were 25% less likely to be readmitted within 30 days. This highlights the critical need for nurses to implement targeted, actionable education that empowers patients to manage their health post-discharge.
To begin, nurses must assess each patient’s health literacy and learning preferences during hospitalization. Use simple language, visual aids, and teach-back methods to ensure comprehension. For example, instead of explaining "hypertension," say, "Your blood pressure is too high, which can harm your heart." Provide written materials in the patient’s preferred language, including step-by-step instructions for self-care tasks like wound dressing or insulin administration. For older adults or those with cognitive impairments, involve family members or caregivers in the education process to reinforce key messages.
Symptom management is another critical area where education can prevent readmissions. Teach patients to recognize early warning signs of deterioration specific to their condition. For a heart failure patient, this might include monitoring daily weight (a sudden increase of 2-3 pounds could indicate fluid retention) and knowing when to adjust diuretic doses under provider guidance. For COPD patients, demonstrate proper inhaler use and explain the difference between manageable shortness of breath and symptoms requiring immediate medical attention, such as bluish lips or severe wheezing.
Equally important is educating patients on when to seek medical attention. Create a personalized "red flag" list tailored to their condition, such as fever above 101°F, persistent vomiting, or chest pain lasting more than 5 minutes. Provide clear instructions on contacting their primary care provider, visiting an urgent care clinic, or calling 911. For example, a patient with diabetes should know that blood sugar levels consistently above 300 mg/dL or below 70 mg/dL warrant immediate action. This specificity reduces hesitation and ensures timely intervention.
Finally, leverage technology to reinforce education post-discharge. Follow-up phone calls or video conferencing within 48 hours of discharge can address lingering questions and assess adherence to care plans. Mobile apps or text message reminders can help patients track medications, symptoms, and appointments. For instance, a pilot program at a Midwestern hospital used automated text reminders for medication adherence, resulting in a 15% reduction in readmissions among participants. By combining in-person education with digital tools, nurses can create a sustainable support system that extends beyond the hospital walls.
Understanding the Role of Hospitals in the US Army Structure
You may want to see also
Explore related products






![]()
Strengthen post-discharge support through home health services, telehealth, and community resource referrals
Hospital readmissions often stem from gaps in care after patients leave the hospital. Strengthening post-discharge support through home health services, telehealth, and community resource referrals can bridge these gaps effectively. Home health services, for instance, provide patients with skilled nursing care, physical therapy, and medication management in the comfort of their homes. A study published in the *Journal of the American Medical Association* found that patients receiving home health care had a 25% lower readmission rate within 30 days compared to those without such support. This approach is particularly beneficial for elderly patients or those with chronic conditions who may struggle with self-care post-discharge.
Telehealth emerges as another critical tool in reducing readmissions by offering remote monitoring and follow-up care. For example, a telehealth program implemented in a rural hospital system used wearable devices to track vital signs like blood pressure and heart rate. Nurses reviewed the data daily and intervened when anomalies were detected, such as a 72-year-old diabetic patient whose elevated blood glucose levels were addressed before complications arose. This proactive approach not only prevented readmissions but also empowered patients to manage their health more effectively. Hospitals can integrate telehealth into discharge plans by providing patients with devices and clear instructions on usage, ensuring seamless continuity of care.
Community resource referrals play a complementary role by addressing social determinants of health that contribute to readmissions. For instance, a patient discharged after a heart attack may need access to affordable healthy food options or transportation to follow-up appointments. Nurses can connect patients with local food banks, meal delivery services, or non-profit transportation programs. A case study from a Midwestern hospital demonstrated that patients referred to community resources had a 40% lower readmission rate compared to those without such referrals. To implement this effectively, hospitals should maintain an updated directory of local resources and train staff to assess patients’ social needs during discharge planning.
Combining these strategies requires a coordinated effort. Start by assessing patients’ post-discharge needs during hospitalization, identifying those at high risk for readmission based on factors like age, comorbidities, and social support. Develop individualized care plans that incorporate home health services, telehealth monitoring, and community resource referrals as needed. For example, a 65-year-old patient with congestive heart failure might receive weekly home health visits, a blood pressure monitor for telehealth tracking, and a referral to a local cardiac support group. Regularly evaluate the effectiveness of these interventions through data analysis, such as tracking readmission rates and patient satisfaction scores, and adjust strategies accordingly. By strengthening post-discharge support in these ways, hospitals can significantly reduce readmissions while improving patient outcomes and quality of life.
VA Hospital CPR Classes: Are They Free in Michigan?
You may want to see also
Explore related products



![]()
Evaluate and refine protocols by tracking readmission data and adjusting strategies based on outcomes
Tracking readmission data is the cornerstone of any initiative aimed at reducing hospital readmissions. Without robust data, it’s impossible to identify trends, pinpoint vulnerabilities, or measure the effectiveness of interventions. Start by establishing a system to collect and analyze readmission rates, segmented by patient demographics, diagnoses, and discharge pathways. For instance, a study published in the *Journal of Nursing Care Quality* found that patients over 65 with chronic conditions like congestive heart failure (CHF) had a 20% readmission rate within 30 days. Such granular data highlights where to focus efforts. Use electronic health records (EHRs) to automate data collection, ensuring accuracy and timeliness. Pair this with regular audits to validate the data and address any gaps.
Once data is collected, the next step is to analyze it for actionable insights. Look for patterns such as frequent reasons for readmission, common complications, or gaps in discharge planning. For example, if data reveals that 30% of CHF readmissions are due to medication non-adherence, this points to a need for improved patient education on diuretic regimens (e.g., furosemide 40 mg twice daily) and follow-up protocols. Comparative analysis can also be powerful: compare readmission rates before and after implementing a transitional care program to gauge its impact. Tools like root cause analysis (RCA) can help dissect complex issues, while dashboards can visualize trends for stakeholders.
Refining protocols based on data insights requires a strategic, iterative approach. Start by piloting small-scale changes in high-risk areas. For instance, if data shows that patients discharged on Fridays have higher readmission rates, consider extending weekend coverage for follow-up calls or clinic hours. Gradually scale successful interventions while monitoring outcomes. Caution: avoid overhauling protocols without evidence. For example, increasing post-discharge home visits for all patients may strain resources without significantly reducing readmissions. Instead, target interventions to specific populations, such as patients with a history of non-adherence or those lacking social support.
Finally, sustain momentum by embedding continuous evaluation into the protocol refinement process. Regularly review readmission data to identify new trends or emerging issues. For instance, if a new medication (e.g., SGLT2 inhibitors for diabetes) is introduced, monitor its impact on readmission rates for patients with comorbidities. Share findings with the interdisciplinary team to foster collaboration and buy-in. Celebrate successes—such as a 15% reduction in readmissions after implementing a medication reconciliation program—to motivate staff. By treating protocol refinement as an ongoing process rather than a one-time fix, nursing teams can adapt to evolving challenges and sustain long-term improvements in patient outcomes.
Hospital Death Protocol: What Happens After a Patient Passes Away?
You may want to see also
Frequently asked questions
Key factors include inadequate patient education, poor care coordination, medication mismanagement, and lack of follow-up care. A nursing project can address these by implementing discharge education programs, enhancing care transitions, using telehealth for follow-ups, and ensuring patients understand their care plans.
Nurses can use teach-back methods to ensure patients understand their discharge instructions, provide written materials in simple language, involve family members in education, and emphasize the importance of medication adherence and symptom monitoring.
Care coordination ensures seamless transitions between hospital and home or other care settings. Nurses can facilitate this by collaborating with primary care providers, arranging timely follow-up appointments, and ensuring all healthcare team members are informed about the patient’s plan of care.
Success can be measured by tracking readmission rates over time, conducting patient satisfaction surveys, monitoring adherence to care plans, and analyzing data on emergency department visits post-discharge. Comparative analysis before and after intervention implementation is also crucial.