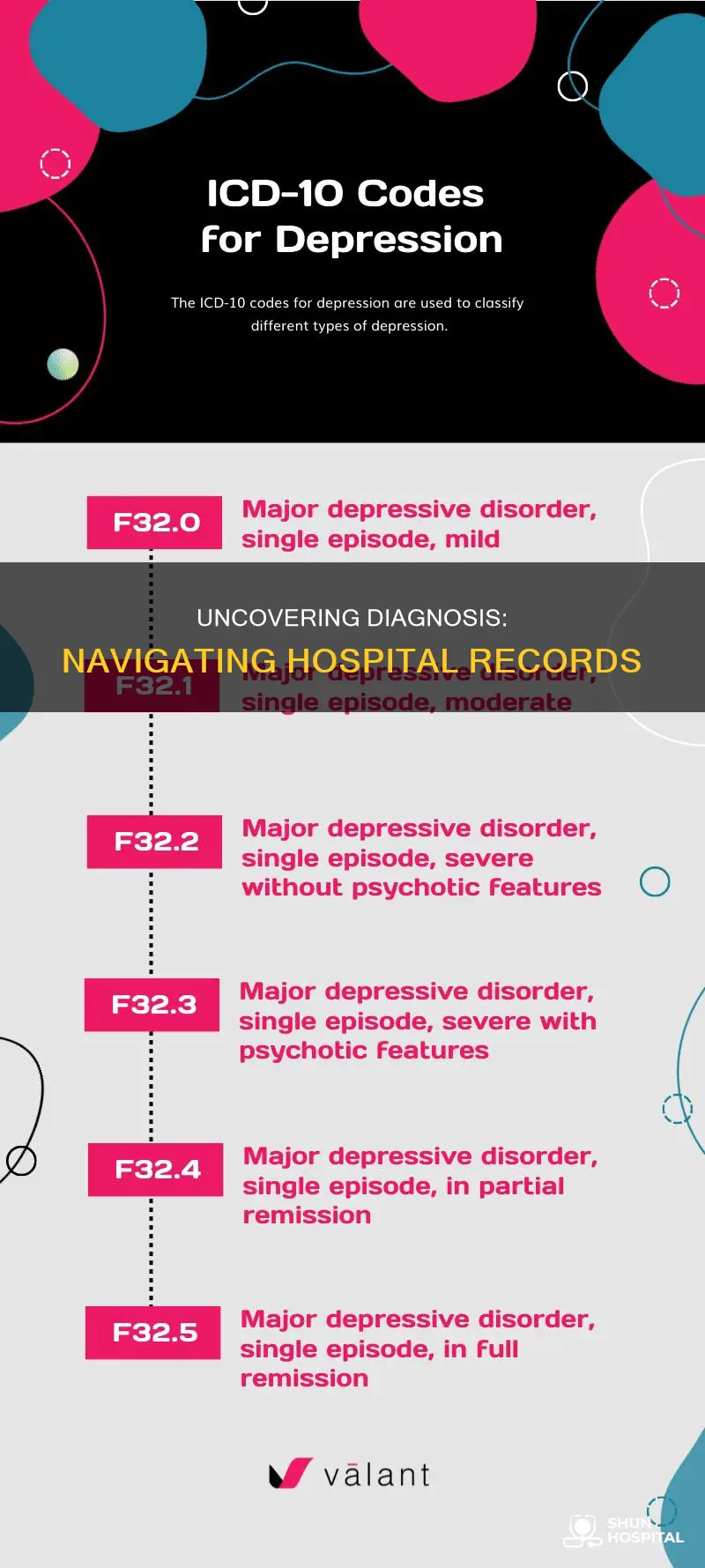
Medical records contain important information about a patient's health, including diagnostic results, medical history, and treatment plans. In many countries, individuals have the right to access and request copies of their medical records, which are often stored electronically. These records can be used to validate diagnoses, conduct research, and inform clinical decision-making. To obtain medical records, individuals can contact their healthcare providers, hospitals, or specialists directly, although access to certain sensitive records, such as mental health notes, may be restricted. It is important to review medical records for accuracy and request corrections if necessary, as errors can impact future health and treatment.
| Characteristics | Values |
|---|---|
| Record Format | Electronic Health Records (EHR) |
| Record Contents | Patient's medical history, diagnostic imaging reports, prescription and dispensing information, hospital discharge summaries, etc. |
| Access | Available to patients, healthcare providers, and authorised representatives. |
| Correction | Patients can request corrections to their records if they find errors or discrepancies. |
| Limitations | May not include older records due to data retention policies and the transition from physical to digital records. |
Explore related products





What You'll Learn
![]()
Requesting hospital records
If you are seeking a specific lab test or hospital record, it is recommended to request them from the facility rather than your primary care provider, as they are more likely to be complete and usually kept for longer. You can request access to your records by checking if your healthcare provider has an online patient portal, which is a secure website where patients can often make appointments, contact their provider, and look at lab results. If they do, you can request your records through this portal. Alternatively, you may have to fill out a health or medical record release form, or request for access, and send it via email, mail, or fax to your provider. You may also be able to request your records via a secure online platform provided by your healthcare provider.
If you are requesting older records, they may be on paper in storage, so it may take some time to find and copy them. After sending in your request, it is a good idea to check with your healthcare provider to ensure they received your request, as sometimes they can get lost. If you have not received your records within 30 days, it is recommended to call again.
If you are requesting records from a hospital, you can submit your request to the facility's Health Information Management (HIM) department. You may need to fill out a Request for Access to Health Information form, which may be organized differently depending on the facility. Some information that you will likely need to include on the form includes the patient's full name, date of birth, patient identification number (PIN), and medical record number (MRN).
If you are requesting that your records be sent to someone other than yourself, you may need to fill out a separate "authorization" form and send it to the relevant department.
The Ultimate Guide to Cleaning Your Hospital Tank
You may want to see also
Explore related products





![]()
Understanding patient privacy rights
In the United States, the Health Insurance Portability and Accountability Act of 1996 (HIPAA) establishes national standards to protect individuals' medical records and other identifiable health information. The HIPAA Privacy Rule, implemented by the Department of Health and Human Services (HHS), sets standards for the protection of health information and provides individuals with privacy rights to understand and control how their health information is used.
Under HIPAA, individuals have the right to inspect, review, and receive a copy of their medical and billing records held by health plans and healthcare providers covered by the Privacy Rule. This includes any diagnostic results, such as blood tests, X-rays, and biopsies. Individuals can also request corrections to their records if they believe the information is incorrect or incomplete. Healthcare providers are required to respond to such requests and make necessary amendments.
However, there are limitations to the records individuals can access. For example, individuals do not have the right to access a provider's psychotherapy notes, which are kept separate from medical and billing records. Additionally, access to mental health records that are considered "impressions" rather than diagnoses may be denied to protect the patient and provider relationship.
To request medical records, individuals can contact the relevant healthcare facility or their healthcare provider. Most providers in the United States are required to retain adult medical records for at least seven years and children's records until the age of majority. Individuals have the right to file a complaint with the Office of Civil Rights (OCR) if they believe their privacy rights have been violated or if they feel they have been unfairly denied access to their records.
Managing Potassium Levels: Hospital Treatment and Care
You may want to see also
Explore related products






![]()
Validating diagnosis in electronic health records
Electronic Health Records (EHR) are electronic systems used and maintained by healthcare systems to collect and store patients' medical information. They contain different types of patient-level variables, such as demographics, diagnoses, problem lists, medications, vital signs, and laboratory data. The adoption of EHR by health services worldwide has facilitated the construction of large population-based patient databases, which have enormous potential for epidemiological and clinical research.
Validating diagnosis in EHR is important to ensure the correctness of the data and make research more credible. Validation of diagnosis algorithms can be done by quantifying the validity of codes and algorithms using diagnostic accuracy test measures. These measures relate what is recorded in the data to a recognised reference standard. The most commonly used and practical of these measures are the positive predictive value (PPV), the negative predictive value (NPV), sensitivity, and specificity.
Another technique to validate diagnosis in EHR is to manually compare a sample of clinical notes in the EHR to the physical chart of the patient. This method was historically used to test EHR reliability when EHR database systems were first implemented. If the physical records accurately reflect the patient's status, this is a reliable way to test the validity of diagnostic codes. However, this approach can be time-consuming and physical records may not always be available, as they are often phased out in favour of digital records.
To assess the "true" disease status of a patient, questionnaires can be sent out to either the patient or the healthcare professional responsible for their care. If an independent secondary database is available, this can also be used to validate diagnostic algorithms, although the results may not be generalisable if the second database does not represent the same population as the first.
Art Therapy: Sending Art to UCSF Hospital
You may want to see also
Explore related products






![]()
Interpreting medical terminology
Familiarize Yourself with the Structure of Medical Records:
Medical records typically include patient information such as name, date of birth, and medical record number. They also contain clinical notes, which summarize symptoms, diagnoses, and treatment plans. Test results, medications, and follow-up instructions are also included in medical records. Understanding the structure of medical records will help you locate relevant information more efficiently.
Learn Common Medical Abbreviations:
Medical reports often contain abbreviations that can be confusing. Familiarize yourself with commonly used abbreviations such as CBC (Complete Blood Count), BP (Blood Pressure), MRI (Magnetic Resonance Imaging), and Rx (Prescription medications). This will help you interpret your records more effectively.
Recognize the Significance of Reference Ranges and Units:
When reviewing test results, pay attention to reference ranges and units. These values provide context for interpreting your results and understanding your health status. Abnormal findings should be discussed with your healthcare provider to ensure a proper understanding of your health condition.
Utilize Digital Tools:
Digital tools, such as patient portals and health analysis applications, can simplify the process of interpreting complex medical data. These tools can help you organize your medical records, track your health progress, and enhance your understanding of your health information.
Maintain Open Communication with Your Healthcare Provider:
While it is important to take an active role in interpreting your medical records, it is equally crucial to maintain open communication with your healthcare provider. They can clarify any confusing terminology, explain the results, and provide insights into your diagnosis and treatment plan. Remember, asking questions enables you to actively participate in your healthcare decisions.
Request Corrections if Necessary:
If you identify any mistakes or outdated information in your medical records, you have the right to request corrections under the HIPAA Privacy Rule. Contact your healthcare provider's office to inquire about their process for updating or correcting medical records. Keeping your records accurate is essential for ensuring effective care and positive health outcomes.
Initiating Hospital Code Green: A Step-by-Step Guide
You may want to see also
Explore related products

$20.77 $114.95





![]()
Correcting errors in records
It is important to correct errors in medical records to ensure quality care and protect patients from harm and legal complications. While many patients are not interested in looking at their own medical records, it is a good idea to do so. According to the Office of the National Coordinator for Health Information Technology, about 1 in 10 people who access records online end up requesting that they be corrected.
Identifying Errors
Common discrepancies may range from personal details to diagnostic annotations. Scrutinize records for any inaccuracies that could hinder care or legal integrity. Typographical errors may or may not require correction. For example, misspelling "mesenteric" as "mesentiric" may not impact your health or medical care. However, errors in the spelling of your name, phone number, or address must be corrected immediately. Failure to do so may result in issues with billing or contacting you about lab results or treatment updates. Any inaccurate information about your symptoms, diagnosis, or treatment should also be corrected.
Requesting Corrections
Once you have identified the errors, you need to request that those mistakes be corrected. Most hospitals, medical offices, or healthcare providers will have a form to fill out, but others may require a written letter. When detailing the errors, be as clear and concise as possible. Include a copy of the pages of your records that contain errors. Then, either mark and fix the mistakes or write a note outlining the corrections. The hospital or medical provider typically has 60 days to act on your request, which can be extended by an additional 30 days. After reviewing your request, they will either accept or deny your changes. If they deny your request, they must notify you of their decision and include both your request and their denial in your medical records.
Correction Process
Healthcare providers must adhere to a definitive protocol when correcting identified mistakes. Once an error has been flagged, the healthcare provider must correct it while keeping the original record intact. This is typically achieved using an annotation or addendum that refers to the incorrect entry. The amendment process must preserve a trace of the original error and the corrected information. This twin documentation serves as a safeguard, providing an apparent historical reference that upholds the integrity of the healthcare record. State laws typically advocate for corrections over erasures, guaranteeing that the original entry remains visible and attributed. Any amendments should be signed and dated to ensure traceability and maintain the standard of care for medical documentation.
What Does Plan F Cover? Deductible and Hospitable Care
You may want to see also
Frequently asked questions
You can request your medical records from your healthcare provider. They may ask you to write a letter or fill out a form. If you think there is a mistake in your records, you have the right to ask your healthcare provider to fix it.
You can access any notes or records that a provider has created, any diagnostic results for which a provider has copies (including blood tests, X-rays, mammograms, etc.), and any information provided by another healthcare provider that was used to establish a diagnosis.
You may be denied access to mental health records that are considered “impressions” rather than diagnoses, as disclosing these may harm the provider-patient relationship if they are misconstrued or taken out of context. However, a provider can only deny access if the information might cause you to hurt yourself or others.
State laws vary, but most providers in the United States are required to keep adult medical records for seven years. The medical records of children must be kept until the age of majority (18 or 21 in most states).































