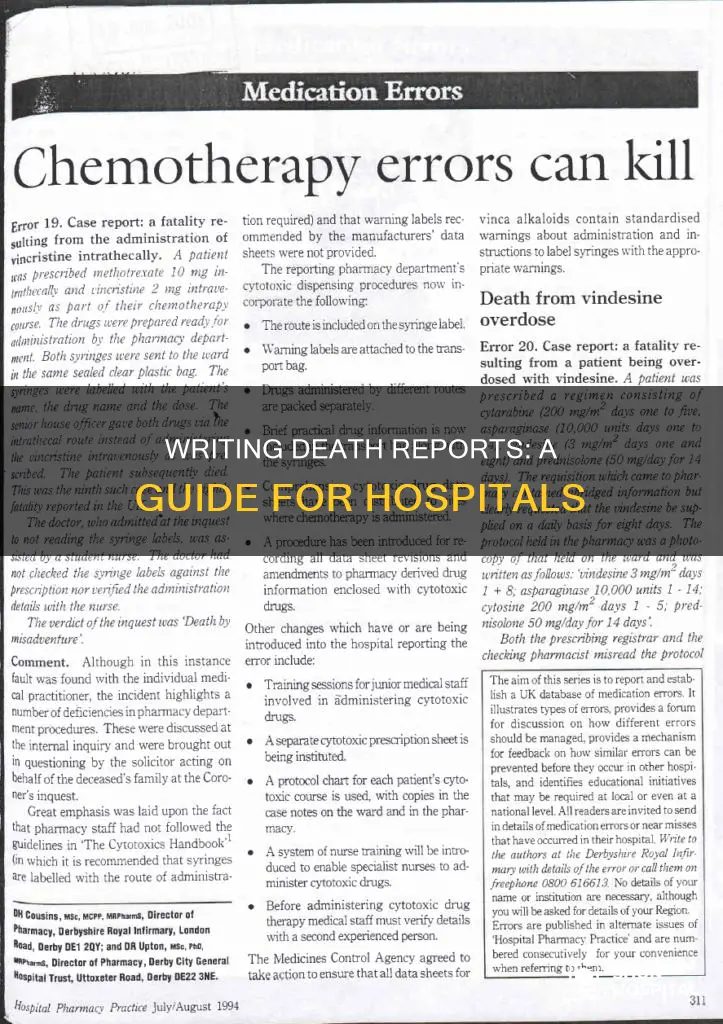
Writing a death report for a hospital patient is a challenging and daunting task for healthcare practitioners and physicians. The death report, also known as a death certificate, must be completed accurately and should include the patient's identifiers, the date and time of death, the cause(s) of death, the outcome of the assessment, and whether an autopsy is accepted or declined by the family. It is important to note that the mechanism of death, such as cardiorespiratory arrest, should not be included in the death report, as it does not specify the cause. Instead, the immediate, intermediate, and underlying causes of death should be listed in sequential order, with the most recent event leading to death listed first.
| Characteristics | Values |
|---|---|
| Writing implement | Pen with black ink |
| Patient identifiers | At least three |
| Reason for attending | Confirm death, reason for death |
| Attendees | Staff members, family, friends |
| Monitoring | ECG, arterial line, echocardiography |
| Observation period | At least five minutes |
| Outcome | Time of death |
| Autopsy | Whether autopsy was accepted or declined |
| Cause of death | Specific, immediate, underlying |
| Contributing factors | Tobacco, alcohol |
| Clinician | Name of clinician completing the certificate |
Explore related products






What You'll Learn
![]()
Use black ink and include patient identifiers
When writing a death report in a hospital setting, it is important to use black ink, as this is the most legible option if notes are photocopied. This is a standard practice for all documentation in a patient's notes.
Additionally, each new sheet of paper should include at least three key identifiers for the relevant patient. This can include the patient's name, age, date of birth, hospital ID, or other unique identifying information. This ensures that the correct patient is identified and that there is no confusion or mix-up of records. If a patient label containing at least three identifiers is readily available, this can be used instead of manually writing out the information on each page.
The patient identifiers are crucial for accurate record-keeping and can help streamline the process of retrieving relevant medical information. It aids in ensuring that the patient's medical history is accurately tracked and that any necessary next steps, such as notifying the family or updating their medical records, can be efficiently undertaken.
Using black ink and including patient identifiers are fundamental steps in maintaining the accuracy and legibility of medical records, specifically in the context of documenting death confirmation and ensuring that the correct patient is identified throughout the process.
State Hospital Commitment: Who Decides?
You may want to see also
Explore related products






![]()
Record time and date of death
Recording the time and date of death is a crucial step in the death reporting process. This information provides an essential timeline of events and helps establish the sequence of actions leading up to and following the death. Here is a detailed guide on recording the time and date of death accurately and comprehensively:
Recording the Time of Death:
When recording the time of death, it is crucial to use the 24-hour clock format, also known as military time. This ensures uniformity and clarity in medical records. For example, if a patient's death occurs at 1 pm, it should be recorded as 13:00 hours. This precise notation eliminates any ambiguity and is the standard format in medical documentation.
Determining the Time of Death:
The determination of the exact time of death is a meticulous process. It involves a comprehensive assessment of the patient, including observing cardiorespiratory functions for at least five minutes. This assessment period is crucial for confirming cardiorespiratory arrest and establishing the time of death. It is important to note that the time of death is documented as the time at which the assessment was completed, signifying the moment when cardiorespiratory functions ceased.
Recording the Date of Death:
Recording the date of death accurately is equally important. The date provides a chronological context for the patient's medical history and the events surrounding their death. The date should be indicated by the day, month, and year. For example, if a patient passes away on January 15, 2023, the date of death should be recorded as 15/01/2023 or January 15, 2023, depending on the preferred format. Consistency in date formatting is crucial to avoid confusion.
Notifying Relevant Parties:
In addition to recording the time and date of death, it is essential to document who was notified about the death. This includes noting whether the family and the attending physician were informed. Clear documentation of notifications ensures that all relevant parties are aware of the patient's passing and can take the necessary steps for the next steps, such as funeral arrangements or further medical procedures.
Correlating Time and Date with Other Information:
Recording the time and date of death accurately is crucial for correlating this information with other medical records. For example, the time and date of death should align with the patient's length of admission, the timeline of their treatment, and the progression of their medical condition. This correlation helps construct a comprehensive overview of the patient's medical history and the circumstances surrounding their death.
London Chest Hospital: Closed or Still Operating?
You may want to see also
Explore related products





![]()
Detail the cause of death
When detailing the cause of death, it is important to be as accurate and specific as possible. The immediate cause of death should be listed first, followed by other contributing conditions in chronological order, ending with the most remote or underlying cause.
For example, a death summary report may list "acute respiratory failure" as the immediate cause of death, followed by "chronic obstructive pulmonary disease exacerbation" as a secondary diagnosis, and then further detail other conditions such as "acute respiratory failure, probably worsened by aspiration", "acute on chronic renal failure", and so on.
In another example, the immediate cause of death could be listed as "cardiopulmonary arrest", with the underlying cause specified as "chronic tissue hypoxia from sickle cell disease". It is important to note that simply listing cardiopulmonary arrest as the cause of death is not sufficient, as it does not specify the underlying condition that led to the arrest.
When filling out the death certificate, it is important to include the length of time between the onset of the condition(s) and death, as well as any contributing factors such as tobacco or alcohol use. If an autopsy is requested, it is advisable to wait for the results before completing the certificate, to ensure accuracy and prevent any discrepancies between the autopsy report and the cause of death listed on the certificate.
Morphine's Impact: Hospital Patient Behavior Explored
You may want to see also
Explore related products






![]()
Note if autopsy accepted or declined
When writing a death report in a hospital, it is important to note whether the family of the deceased has accepted or declined an autopsy. An autopsy is a medical examination of a body after death, and it serves as a powerful diagnostic tool to determine the cause and mode of death. It can also provide valuable insights into the pathological processes involved and identify any contributory factors, such as infectious diseases.
The decision to accept or decline an autopsy rests with the family of the deceased. In some cases, the family may decline the autopsy due to cultural or religious beliefs, or they may feel that it will cause additional suffering. Additionally, the family may consider the cost of the procedure or believe that there is no new knowledge to be gained from it. It is important to respect the family's decision and document their choice in the death report.
If the autopsy is accepted, the report should include details about the process and the findings. The report should mention the type of autopsy performed, such as a forensic autopsy or a clinical medical autopsy, and the name of the pathologist or medical examiner who conducted the procedure. It is standard practice to include the date and time the autopsy was performed and a detailed description of the external and internal examination of the body. Any toxicology reports, biochemical tests, or genetic testing results that were part of the autopsy should also be included in the report.
In some cases, the family may request a second autopsy if they are unsure about the findings or want further clarification. This request should also be documented in the death report, along with the reason for the request and the name of the new pathologist or medical examiner involved.
Inova: Academic or Community Hospital?
You may want to see also
Explore related products





![]()
Confirm if coroner was notified
When writing a death report in a hospital setting, it is important to confirm whether the coroner was notified. This step is crucial to ensure compliance with legal requirements and to provide accurate documentation of the death. Here are some detailed instructions on how to confirm if the coroner was notified:
Firstly, it is essential to understand the role of the coroner in the context of a hospital death. The coroner is responsible for investigating and confirming the cause of death, particularly in cases where the death was unexpected, unnatural, or occurred without medical attendance. The coroner may order a post-mortem examination or an inquest to determine the cause of death if it cannot be certified by a doctor.
In most cases, hospital doctors, out-of-hours doctors, or GPs are responsible for reporting a death to the coroner. This reporting usually occurs when the cause of death is unclear, or if the death was unexpected or unnatural. The relevant parties should confirm if the death has been reported to the coroner and if an investigation has been initiated. This information can be obtained by contacting the coroner's office or the police, who are typically involved in gathering information about the death.
Additionally, it is important to review the patient's medical records and charts. These documents should indicate whether the coroner was notified and provide details about any interactions or communications with the coroner's office. The medical records may also contain information about the cause of death, which can help determine if a coroner's involvement is necessary.
Another aspect to consider is the presence of the patient's family members. In some cases, family members may have been in contact with the coroner's office, especially if they were involved in the decision-making process regarding post-mortem examinations or inquests. Discussing the matter with the family can help confirm if the coroner has been notified and provide additional insights into the process.
Lastly, it is crucial to follow up with the relevant hospital staff, including nurses and physicians, who were involved in the patient's care. They may have direct knowledge or documentation indicating whether the coroner was notified. This step helps ensure that all necessary procedures were followed and that the death report is comprehensive and accurate. By following these steps, you can confirm if the coroner was notified and gather the necessary information for a complete and compliant death report in a hospital setting.
Stanford Hospital: Santa Clara County's Top-Rated Medical Center
You may want to see also