Hyperglycemia, defined as a blood glucose level greater than 140 mg/dL, is reported in 22-46% of non-critically ill hospitalized patients. It is associated with an increased risk of complications and mortality, especially in patients without a history of diabetes. The management of hyperglycemia in hospitals involves identifying blood glucose targets, using oral diabetes medications or insulin therapy, and implementing glycemic control protocols. Hospitals have developed protocols for managing hyperglycemia and hypoglycemia, with a focus on prompt treatment and interdisciplinary collaboration. Continuous glucose monitoring systems and diabetes self-management education are also employed to improve inpatient care and reduce readmissions. The target blood glucose range for hospitalized patients is typically between 140 and 180 mg/dL, with adjustments made based on individual clinical situations.
| Characteristics | Values |
|---|---|
| Definition of hyperglycemia | Blood glucose level greater than 140 mg/dL (7.8 mmol/L) |
| Prevalence | Affects 537 million adults globally, including 38.1 million in the US |
| Hospitalization rate | Patients with diabetes have a 3-4 times higher chance of hospitalization |
| Inpatient hyperglycemia | Associated with increased risk of complications and mortality |
| Treatment | Correctional insulin, scheduled insulin therapy, dipeptidyl peptidase inhibitors, continuous glucose monitoring, insulin pump therapy, diabetes self-management education |
| Risk factors for hypoglycemia | Age, BMI, total daily insulin dose, history of chronic kidney disease, liver failure, cerebrovascular accident, active malignancy, pancreatic disorders, congestive heart failure, infection, history of hypoglycemia |
| Protocols | Identifying risk factors, implementing protocols, avoiding sliding scale insulin regimens, changing unsafe prescribing behaviors, early detection, treatment and monitoring, interdisciplinary protocol development |
| Glucose targets | Flexible targets based on individual clinical situations, current target range of 140-180 mg/dL |
| Challenges | Identifying blood glucose targets, judicious use of oral diabetes medications, implementing appropriate insulin regimens |
| Complications | Poor wound healing, increased risk of infection, delays in surgical procedures or hospital discharge |
Explore related products





What You'll Learn
![]()
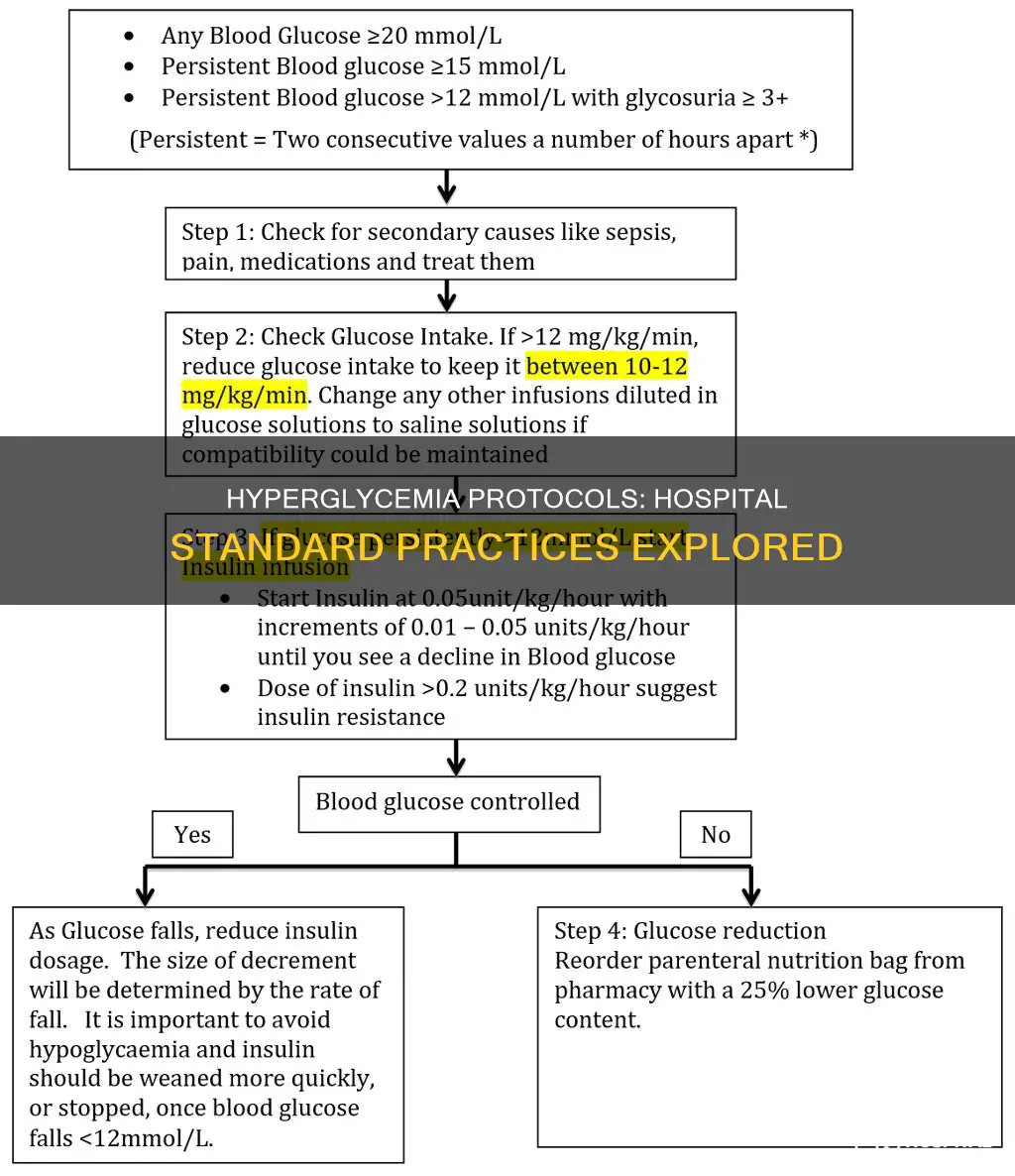
Hyperglycemia treatment: intravenous insulin infusion
Hyperglycemia is defined as a blood glucose level greater than 140 mg/dL (7.8 mmol/L) and is reported in 22-46% of non-critically ill hospitalized patients. It is associated with an increased risk of complications and mortality in patients with or without a prior diabetes diagnosis.
Intravenous insulin infusions are an effective way to manage hyperglycemia in hospital settings. They are often used in patients with hyperglycemia who have suboptimal glucose control with conventional subcutaneous insulin treatment. Intravenous insulin infusions can also be used to control hyperglycemia in patients who have undergone open cardiac surgery due to their susceptibility to deep wound infections.
The Society of Critical Care Medicine (SCCM) recommends initiating glycemic management protocols to treat persistent hyperglycemia greater than or equal to 180 mg/dL (10 mmol/L) to maintain target glucose levels below 180 mg/dL in critically ill adults. This can be achieved through Variable Rate Insulin Infusion (VRII), which involves adjusting the rate of insulin infusion according to regular capillary blood glucose measurements. The optimal glycemic target for critically ill patients is generally considered to be between 140 and 180 mg/dL (7.8-10.0 mmol/L).
Intravenous insulin infusion preparation involves adding 50 units of regular insulin to 50 ml of normal saline to achieve a final concentration of 1 unit/ml. Once the infusion is initiated, the titration will depend on multiple variables, including the current blood glucose level, target blood glucose level, rate of blood glucose change, and meal timing and content.
It is important to closely monitor and adjust insulin dosing to avoid complications such as hypoglycemia, which is associated with an increased risk of death in diabetic patients.
MRI Availability at Valley View Hospital
You may want to see also
Explore related products






![]()
Diabetes self-management education
Diabetes is a complex metabolic disorder that affects how the body turns food into energy. It is a highly prevalent condition, with an estimated 537 million adults affected worldwide in 2021. People with diabetes have a 3-4 times greater chance of requiring hospitalisation, and inpatient hyperglycemia is associated with an increased risk of complications and mortality.
- Healthy eating
- Being active
- Taking medication as prescribed
- Monitoring blood sugar levels, activity, and eating habits
- Reducing risks to prevent diabetes complications
- Healthy coping strategies for emotional well-being
- Problem-solving to find solutions and take action
DSMES aims to improve clinical care and education services, enhance individuals' health, and reduce diabetes-associated healthcare costs. It empowers individuals to fit diabetes care into their daily lives, promoting effective self-management. DSMES can be accessed through various settings, including hospital outpatient centres, clinics, physicians' offices, and wellness centres, with many programs accredited by organisations like ADCES®.
In the context of hospitals, inpatient hyperglycemia guidelines emphasise the use of emerging diabetes technology and insulin therapy for glycemic management. Continuous glucose monitoring systems can help achieve glycemic targets and reduce hypoglycemia risks. For instance, patients with newly recognised hyperglycemia may be treated with correctional insulin alone upon hospital admission. Additionally, diabetes self-management education can lead to improved glycemic control and reduced hospital readmission rates.
Large Hospitals: Embracing Telemedicine's Future
You may want to see also
Explore related products





![]()
Inpatient hyperglycemia: risk factors
Hyperglycemia is defined as a blood glucose level greater than 140 mg/dL (7.8 mmol/L) and is reported in 22-46% of non-critically ill hospitalized patients. Inpatient hyperglycemia is associated with an increased risk of complications, mortality, longer hospital stays, a higher admission rate to the intensive care unit (ICU), and a higher need for transitional or nursing home care after hospital discharge. Several risk factors have been identified for inpatient hyperglycemia:
Risk Factors for Inpatient Hyperglycemia
- Diabetes: Patients with diabetes have a 3-4 times greater chance of hospitalization and longer hospital stays. Diabetes is a metabolic disorder that affects blood glucose regulation, leading to hyperglycemia.
- Stress Hyperglycemia: Inpatient hyperglycemia can occur in patients with or without a prior diagnosis of diabetes, including those with stress-induced hyperglycemia or previously undiagnosed diabetes.
- Glucocorticoid Therapy: Patients receiving glucocorticoid therapy or enteral nutrition are at high risk for hyperglycemia and require scheduled insulin therapy in the hospital.
- Age: Older patients are at a higher risk of developing hyperglycemia during hospitalization.
- Illness Severity: The severity of illness before or during hospitalization can impact blood glucose levels and contribute to hyperglycemia.
- Comorbidities: Multiple comorbid diseases increase the risk of inpatient hyperglycemia and can complicate its management.
- BMI: A lower body mass index (BMI) is associated with a higher risk of hyperglycemia.
- Prior Hypoglycemia: A history of hypoglycemia, either before or during hospitalization, is a risk factor for inpatient hyperglycemia.
- Medication Interactions: Concurrent use of certain drugs with hypoglycemic agents, such as warfarin, quinine, or salicylates, can increase the risk of hyperglycemia.
- Inadequate Glucose Monitoring: Inadequate or unclear physician instructions, limited health personnel, or interruptions in established glucose monitoring routines can contribute to the risk of hyperglycemia.
- Nutritional Factors: Unexpected changes in nutritional intake, such as cessation of nutrition for procedures or adjustments in nutritional support, can impact blood glucose levels and lead to hyperglycemia.
- Steroid Therapy: Tapering of steroid therapy or the use of certain steroids, such as prednisolone or dexamethasone, can contribute to the development of hyperglycemia.
Hospital Backup Generators: Are They Mandatory?
You may want to see also
Explore related products






![]()
Protocols for treating hyperglycemia
Hyperglycemia, defined as a blood glucose level greater than 140 mg/dL (7.8 mmol/L), is observed in 22-46% of non-critically ill hospitalised patients. It is associated with an increased risk of complications and mortality, especially in patients without a history of diabetes.
The Society of Critical Care Medicine (SCCM) guidelines recommend that clinicians initiate glycemic management protocols to treat hyperglycemia in critically ill patients. This includes the use of insulin infusion to maintain blood glucose levels below 180 mg/dL (10 mmol/L). The SCCM guidelines also suggest designing the insulin regimen and monitoring system to avoid and detect hypoglycemia (blood glucose <70 mg/dL or <3.9 mmol/L).
Several insulin infusion protocols are effective in achieving glycemic control and reducing hypoglycemic events in hospitalised patients. These protocols should be flexible and allow for modifications based on individual clinical situations. They should also provide clear instructions on the blood glucose threshold for initiating insulin infusion and the initial rate of administration.
In patients with newly recognised hyperglycemia or well-managed diabetes on non-insulin therapy, correctional insulin alone may be used as initial therapy. For patients with persistent blood glucose values above 180 mg/dL, scheduled insulin therapy is preferred. Continuous glucose monitoring systems can help achieve glycemic targets and reduce hypoglycemia. Computer-based algorithms that guide nursing staff in adjusting insulin infusion rates have been shown to provide tighter glycemic control than standard paper form protocols.
Additionally, diabetes self-management education for hospitalised patients can improve glycemic control and reduce the risk of hospital readmission. This includes comprehensive education on self-monitoring of blood glucose, diet, injection technique, self-titration of insulin, and the prevention and treatment of hypoglycemia.
Reverse Shoulder Replacement: Hospital Stay Needed?
You may want to see also
Explore related products






![]()
Glucose targets and insulin regimens
The management of hyperglycemia in hospitals involves the use of various insulin regimens and glucose targets to maintain blood glucose levels within a safe range. The specific targets and treatments can vary depending on the patient's condition and the hospital's protocols. Here is an overview of the glucose targets and insulin regimens commonly used in hospitals:
Glucose Targets:
- The Society of Critical Care Medicine (SCCM) guidelines recommend maintaining blood glucose levels below 180 mg/dL (10.0 mmol/L) in critically ill adults.
- The American Diabetes Association (ADA) suggests a glycemic goal of 140–180 mg/dL (7.8–10.0 mmol/L) for patients with diabetes.
- The JBDS Inpatient Care group in the UK recommends a target range of 6.0–10.0 mmol/L (108–180 mg/dL) for inpatients with hyperglycemia, with an acceptable range of 4.0–12.0 mmol/L (72–216 mg/dL).
- For patients with ischaemic events, a lower glucose range of 100–140 mg/dL may be targeted to reduce potential harms associated with hyperglycemia.
Insulin Regimens:
- Basal-Bolus Correctional Approach: This strategy involves using long-acting insulin along with adjusted premeal short-acting insulin. It addresses basal, nutritional, and supplemental insulin requirements.
- Sliding Scale Insulin Regimens: While historically used, these regimens are not recommended due to their inability to control glucose levels proactively and the risk of wide fluctuations in blood glucose levels.
- Intravenous Insulin Infusion: For patients with severe hyperglycemia, an intravenous insulin infusion is often started to rapidly bring blood glucose levels under control.
- Continuous Insulin Infusion Therapy: This is the preferred regimen for ICU patients with hyperglycemia and those with hyperglycemic crises.
- Correctional Insulin Alone: Patients with newly recognized hyperglycemia or well-managed diabetes may be treated with correctional insulin as initial therapy.
- Basal-Plus Approach: This regimen is suitable for patients with mild hyperglycemia, decreased oral intake, or those undergoing surgery. It involves a single dose of basal insulin along with corrective doses before meals or every 6 hours.
- Neutral Protamine Hagedorn (NPH) Insulin Regimens: These are used in specific cases, such as for patients receiving corticosteroids or those with diabetes undergoing surgery.
The choice of insulin regimen depends on the patient's condition, the severity of hyperglycemia, and the clinical judgment of the treating physicians. Continuous glucose monitoring systems and diabetes self-management education can also play a role in achieving glycemic targets and improving patient outcomes.
Exploring New York's Extensive Hospital Network
You may want to see also
Frequently asked questions
Hyperglycemia is defined as a blood glucose level greater than 140 mg per dL (7.8 mmol per L).
Hyperglycemia is associated with an increased risk of complications and mortality, especially in patients without a history of diabetes. It can also lead to poor wound healing, an increased risk of infection, and delays in surgical procedures or hospital discharge.
The treatment for hyperglycemia in hospitals typically involves initiating a variable rate intravenous insulin infusion to maintain blood glucose levels below 180 mg/dL. This is done in conjunction with monitoring blood glucose levels, providing patient education, and ensuring proper nutrition.
Yes, the Society of Critical Care Medicine (SCCM) guidelines recommend against titrating insulin infusion to a lower glucose target of 80-139 mg/dL for critically ill patients. Instead, they advise maintaining a target glucose level below 180 mg/dL.
Hypoglycemia, defined as a blood glucose level less than 70 mg/dL, can be prevented by recognizing risk factors, implementing standard protocols, avoiding sliding scale insulin regimens, and ensuring proper nutrition and medication management. Prompt treatment is crucial upon identification.