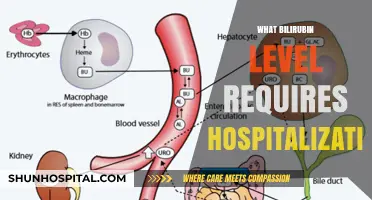
When considering whether a Body Mass Index (BMI) requires hospitalization, it’s important to understand that BMI alone is not a definitive indicator of health or the need for medical intervention. However, extremely high or low BMI values can signal severe health risks that may necessitate hospitalization. For instance, a BMI below 15 often indicates severe malnutrition or anorexia nervosa, which can lead to life-threatening complications such as organ failure or cardiac issues, requiring immediate medical attention. On the other hand, a BMI above 40 (classified as morbid obesity) may lead to critical conditions like severe sleep apnea, heart disease, or diabetes, which could warrant hospitalization for stabilization or surgical interventions like bariatric surgery. Ultimately, hospitalization is determined by the presence of associated medical complications rather than BMI alone, though extreme values often serve as a red flag for urgent evaluation and care.
Explore related products






What You'll Learn
- BMI Thresholds for Hospitalization: Specific BMI levels that necessitate immediate medical attention and hospitalization
- Health Risks at Extreme BMI: Severe complications linked to critically high or low BMI values
- Hospitalization for BMI-Related Conditions: Treatment of obesity or malnutrition-induced health issues requiring inpatient care
- Emergency BMI Interventions: Urgent medical procedures for life-threatening BMI-related conditions like organ failure
- BMI and Mental Health Hospitalization: Psychiatric care for eating disorders tied to extreme BMI levels
![]()
BMI Thresholds for Hospitalization: Specific BMI levels that necessitate immediate medical attention and hospitalization
Body Mass Index (BMI) serves as a critical indicator of overall health, but certain thresholds signal the need for immediate medical intervention. A BMI below 15 in adults is widely recognized as a severe health risk, often necessitating hospitalization. At this level, individuals face life-threatening complications such as organ failure, severe malnutrition, and compromised immune function. For context, a BMI of 15 corresponds to a 5’4” adult weighing approximately 95 pounds. Immediate hospitalization is essential to address nutritional deficiencies, stabilize vital functions, and prevent irreversible damage.
While extremely low BMI values are more commonly associated with hospitalization, dangerously high BMIs also warrant urgent care. A BMI exceeding 60, though rare, indicates severe obesity that can lead to critical conditions like respiratory failure, cardiovascular collapse, or multiple organ dysfunction syndrome. Patients with such extreme BMIs often require intensive monitoring, specialized equipment, and multidisciplinary interventions. For instance, bariatric surgery or weight management programs may be initiated in a hospital setting to mitigate risks and improve long-term outcomes.
Pediatric cases introduce additional complexity, as BMI thresholds for hospitalization vary by age and developmental stage. In children, a BMI below the 1st percentile or above the 99th percentile for their age group raises significant concern. Hospitalization may be required for comprehensive evaluation, nutritional support, or psychological intervention, particularly in cases of eating disorders or obesity-related comorbidities. Early intervention is crucial to prevent stunted growth, developmental delays, or chronic health issues later in life.
Practical considerations for healthcare providers include recognizing red flags such as rapid weight changes, syncope, or unexplained fatigue, which may precede critical BMI thresholds. Hospitalization protocols should prioritize stabilizing the patient, addressing underlying causes, and creating a tailored treatment plan. For example, nasogastric feeding or total parenteral nutrition may be employed for severe malnutrition, while mechanical ventilation could be necessary for obesity-related respiratory distress. Collaboration among dietitians, psychologists, and medical specialists ensures holistic care during and after hospitalization.
In summary, specific BMI thresholds—such as below 15 or above 60 in adults, and extreme percentiles in children—demand immediate hospitalization to avert severe health consequences. Recognizing these critical values and understanding the associated risks enables timely, effective interventions. Whether addressing malnutrition or morbid obesity, hospitalization serves as a lifeline, offering intensive care and resources to restore health and prevent long-term complications.
Meet the CEO Leading Holly Hill Hospital's Healthcare Innovations
You may want to see also
Explore related products






![]()
Health Risks at Extreme BMI: Severe complications linked to critically high or low BMI values
Extreme BMI values, whether critically high or low, signal a body under siege, pushing physiological limits to the brink. A BMI below 15 or above 40 often correlates with severe malnutrition or morbid obesity, respectively, both of which can trigger life-threatening complications. At these extremes, the body’s ability to maintain homeostasis collapses, leading to organ failure, immune dysfunction, and metabolic chaos. Hospitalization becomes not just likely but necessary to stabilize the patient and prevent irreversible damage.
Consider the case of severe anorexia nervosa, where a BMI below 13 can result in bradycardia, hypotension, and electrolyte imbalances, particularly hypokalemia and hypophosphatemia. These conditions are not merely inconvenient; they are lethal without intervention. Similarly, a BMI exceeding 50 in obesity often leads to severe complications like obstructive sleep apnea, pulmonary hypertension, and type 2 diabetes with ketoacidosis. Each of these conditions demands immediate medical attention, often requiring intensive monitoring and multimodal treatment plans.
For individuals with critically low BMI, refeeding syndrome poses a unique danger during hospitalization. Rapid nutrient replenishment can trigger fatal shifts in fluid and electrolyte balance, necessitating slow, controlled refeeding protocols. Patients with a BMI below 12, for instance, may require initial caloric intake as low as 5–10 kcal/kg/day, gradually increasing by 20% every 2–3 days under strict medical supervision. Conversely, those with morbid obesity (BMI >45) often face surgical interventions like bariatric surgery, which carries its own risks, including nutrient deficiencies and postoperative complications such as leaks or infections.
The psychological toll of extreme BMI cannot be overlooked. Severe obesity is frequently accompanied by depression, anxiety, and social isolation, while anorexia nervosa and other eating disorders are often rooted in deep-seated psychological trauma. Hospitalization in these cases must include psychiatric evaluation and therapy, alongside physical treatment. For example, cognitive-behavioral therapy (CBT) has proven effective in addressing disordered eating patterns, while support groups provide a sense of community and accountability.
Ultimately, hospitalization for extreme BMI is not merely about correcting a number on a scale. It’s about addressing a systemic breakdown that affects every organ, every cell, and every aspect of a person’s life. Whether through meticulous nutritional rehabilitation, surgical intervention, or psychological support, the goal is to restore not just physical health but also the quality of life. Ignoring these critical thresholds risks not only hospitalization but also long-term disability or death, making early intervention and comprehensive care non-negotiable.
Hospitality Suite: Conference Networking Powerhouse
You may want to see also
Explore related products





![]()
Hospitalization for BMI-Related Conditions: Treatment of obesity or malnutrition-induced health issues requiring inpatient care
Extreme BMI values, whether indicative of severe obesity or malnutrition, often necessitate hospitalization due to the critical health complications they trigger. For instance, a BMI exceeding 40 in adults significantly increases the risk of conditions like type 2 diabetes, hypertension, and obstructive sleep apnea, which may require inpatient management. Similarly, a BMI below 16 in adults or below the 3rd percentile in children signals severe malnutrition, leading to life-threatening issues such as organ failure or immune dysfunction. Hospitalization in these cases is not about the BMI number itself but about addressing the cascading health crises it represents.
In the case of severe obesity, hospitalization often involves multidisciplinary care to stabilize acute complications. For example, patients with BMI-related heart failure may receive diuretics (e.g., furosemide 40–80 mg/day) to manage fluid overload, alongside telemetry monitoring for arrhythmias. Bariatric surgery, such as gastric bypass or sleeve gastrectomy, may be considered for those with a BMI over 50 or BMI over 35 with comorbidities, but only after thorough preoperative evaluation. Post-surgery, patients require close monitoring for complications like leaks or nutrient deficiencies, emphasizing the inpatient setting’s role in ensuring safety and efficacy.
Malnutrition-induced hospitalizations, on the other hand, focus on refeeding protocols and addressing underlying causes. Patients with severe malnutrition (BMI < 16) are at risk of refeeding syndrome, a potentially fatal condition caused by rapid electrolyte shifts. Treatment includes gradual calorie reintroduction (starting at 10–15 kcal/kg/day) and close monitoring of phosphorus, magnesium, and potassium levels, with supplementation as needed. For children, age-specific formulas like Pediasure (1.0 kcal/mL) or specialized feeds may be used, alongside psychological support for conditions like anorexia nervosa, which often underlie malnutrition in adolescents.
Comparing the two extremes, obesity and malnutrition hospitalizations differ in approach but share a focus on systemic stabilization. While obesity treatment leans toward surgical and pharmacological interventions, malnutrition care prioritizes nutritional rehabilitation and psychological therapy. Both require tailored plans: obese patients may need mobility aids and pressure ulcer prevention, while malnourished individuals often require feeding tubes or TPN (total parenteral nutrition) if oral intake is insufficient. The goal in both cases is not just BMI adjustment but restoring functional health and preventing long-term complications.
Practical tips for caregivers include recognizing early warning signs: unexplained weight loss or gain, fatigue, and changes in skin integrity. For obese patients, encourage gradual weight loss (1–2 pounds/week) through diet and exercise before complications arise. For malnourished individuals, ensure high-calorie, nutrient-dense meals and monitor for signs of refeeding syndrome during recovery. Hospitalization should be viewed as a last resort but a critical intervention when outpatient management fails, offering specialized care to address the complex interplay of BMI-related health issues.
Seeking Psychiatric Help: Checking into a Hospital
You may want to see also
Explore related products






![]()
Emergency BMI Interventions: Urgent medical procedures for life-threatening BMI-related conditions like organ failure
A Body Mass Index (BMI) below 15 or above 40 often signals a critical health crisis requiring immediate hospitalization. At these extremes, the body’s systems begin to fail, leading to organ dysfunction, severe malnutrition, or life-threatening complications like heart failure or respiratory distress. Emergency BMI interventions are not elective procedures but urgent, life-saving measures designed to stabilize the patient and prevent irreversible damage. These interventions often involve a multidisciplinary approach, combining medical, nutritional, and psychological strategies to address the root causes and immediate dangers.
Consider a patient with a BMI of 12 due to anorexia nervosa, presenting with bradycardia, hypotension, and electrolyte imbalances. Immediate hospitalization is mandatory, starting with intravenous fluids to correct dehydration and electrolyte abnormalities. Nasogastric feeding may be initiated if oral intake is unsafe, delivering 20–30 kcal/kg/day initially, gradually increasing to 50–80 kcal/kg/day as tolerated. Cardiac monitoring is essential, as refeeding syndrome—a potentially fatal condition marked by fluid and electrolyte shifts—can occur within 3–5 days of refeeding. This example underscores the precision required in emergency BMI interventions, balancing rapid nutritional support with careful monitoring to avoid complications.
In contrast, a patient with a BMI of 60 may face equally dire risks, such as acute respiratory distress syndrome (ARDS) or decompensated heart failure. Hospitalization often involves intensive care unit (ICU) admission, with interventions like non-invasive ventilation or continuous positive airway pressure (CPAP) to support breathing. Diuretics, such as furosemide (40–80 mg IV), may be administered to reduce fluid overload, while inotropic support like milrinone (0.375–0.75 mcg/kg/min) can stabilize cardiac function. Bariatric surgery, such as sleeve gastrectomy or gastric bypass, may be considered as a last resort, but only after stabilizing the patient’s acute condition. This comparative approach highlights the divergent yet equally urgent needs of patients at opposite BMI extremes.
Practical tips for healthcare providers include early involvement of dietitians, psychologists, and specialists in critical care. For severely underweight patients, avoid abrupt dietary changes and monitor for refeeding syndrome with daily electrolyte checks. For morbidly obese patients, ensure equipment and facilities can accommodate their size, from reinforced beds to specialized imaging machines. Families should be educated on the risks of extreme BMI and the importance of compliance with treatment plans. These interventions are not just medical procedures but a lifeline, requiring swift action and meticulous care to restore health and prevent tragedy.
Hospital Stays and Cholesterol: Understanding the Impact on Your Levels
You may want to see also
Explore related products





![]()
BMI and Mental Health Hospitalization: Psychiatric care for eating disorders tied to extreme BMI levels
Extreme BMI levels, particularly those below 13 or above 40, often signal a critical need for hospitalization. However, when discussing BMI and mental health hospitalization, the focus shifts to eating disorders, where psychiatric care becomes paramount. For individuals with anorexia nervosa, a BMI below 15 is a red flag, often necessitating immediate medical intervention due to the heightened risk of organ failure, electrolyte imbalances, and cardiac complications. Hospitalization in these cases isn’t just about stabilizing physical health; it’s about addressing the psychological underpinnings of the disorder through therapy, nutritional counseling, and medication management.
Contrastingly, binge-eating disorder or bulimia nervosa may not always present with extremely low BMIs, but severe cases can lead to obesity-related complications, such as type 2 diabetes or cardiovascular issues, requiring hospitalization. Here, psychiatric care focuses on breaking the cycle of binge-purge behaviors or emotional eating through cognitive-behavioral therapy (CBT) and dialectical behavior therapy (DBT). Hospitalization provides a structured environment to monitor physical health while addressing the mental health triggers that perpetuate the disorder.
A critical aspect of BMI-related hospitalization for eating disorders is the multidisciplinary approach. Patients often require a team of dietitians, psychiatrists, and primary care physicians to address both the physical and psychological dimensions of their condition. For instance, refeeding syndrome—a life-threatening condition caused by rapid nutritional rehabilitation in severely malnourished individuals—requires careful monitoring of electrolytes and gradual calorie increases, typically starting at 1000 kcal/day and increasing by 200–400 kcal every 2–3 days.
Age plays a significant role in treatment strategies. Adolescents with eating disorders often require family-based therapy (FBT), where parents take an active role in meal planning and supervision. Adults, on the other hand, may benefit from individual psychotherapy or group therapy sessions. Regardless of age, hospitalization aims to restore medical stability, normalize eating patterns, and equip patients with coping mechanisms to prevent relapse.
Practical tips for caregivers and patients include maintaining open communication, avoiding judgmental language, and focusing on behaviors rather than weight. For those transitioning from hospital to outpatient care, creating a structured daily routine and identifying early warning signs of relapse are crucial. Ultimately, BMI serves as a critical but incomplete indicator of health in the context of eating disorders; hospitalization is a lifeline that integrates physical and mental health care to foster recovery.
Exploring Soweto's Healthcare: A Comprehensive Guide to Local Hospitals
You may want to see also
Frequently asked questions
A BMI below 15 or above 40 often requires hospitalization due to severe health risks associated with extreme underweight or obesity.
A BMI of 30 (obesity) may require hospitalization if it leads to severe complications like heart disease, diabetes, or respiratory issues.
A BMI of 16 (severe thinness) often requires hospitalization due to malnutrition, organ failure, or other life-threatening conditions.
A BMI of 45 (morbid obesity) may require hospitalization for issues like severe sleep apnea, mobility limitations, or critical metabolic disorders.


![South Park: The End of Obesity [Blu-Ray]](https://m.media-amazon.com/images/I/41ilBByn6uL._AC_UL320_.jpg)






![Obesity Medicine Board Review Questions 2025 [ABOM Inspired]: 575+ In-Depth Q&A to Ensure Your Exam Success](https://m.media-amazon.com/images/I/61Zu-Q+yJeL._AC_UL320_.jpg)