Being hospitalized for alcohol withdrawal is a challenging and often necessary step for individuals whose bodies have become dependent on alcohol. The experience typically begins with an assessment by medical professionals to determine the severity of withdrawal symptoms, which can range from mild anxiety and tremors to severe complications like seizures or delirium tremens (DTs). Patients are closely monitored in a controlled environment, where medications such as benzodiazepines may be administered to manage symptoms and prevent life-threatening complications. The hospital setting provides not only physical safety but also emotional support, as withdrawal can be emotionally taxing, with feelings of anxiety, depression, and restlessness being common. The process often includes counseling or therapy to address the underlying issues contributing to alcohol dependence, laying the groundwork for long-term recovery. While the experience can be daunting, hospitalization offers a critical opportunity for stabilization, healing, and a fresh start toward sobriety.
| Characteristics | Values |
|---|---|
| Severity of Symptoms | Ranges from mild (anxiety, tremors) to severe (seizures, delirium tremens). |
| Duration of Hospitalization | Typically 3–7 days, depending on symptom severity and complications. |
| Medical Monitoring | Continuous vital sign monitoring (heart rate, blood pressure, temperature). |
| Medications Administered | Benzodiazepines (e.g., diazepam), antipsychotics, and anticonvulsants. |
| IV Fluids and Electrolyte Management | Administered to address dehydration and electrolyte imbalances. |
| Psychological Support | Counseling, therapy, and support groups for emotional and mental health. |
| Physical Environment | Quiet, controlled hospital setting with minimal stimuli to reduce stress. |
| Withdrawal Timeline | Symptoms peak within 24–72 hours, with gradual improvement thereafter. |
| Risk of Complications | High risk of seizures, dehydration, malnutrition, and delirium tremens. |
| Discharge Planning | Includes referrals to rehab, outpatient treatment, and aftercare programs. |
| Patient Experience | Often described as physically and emotionally challenging but necessary. |
| Success Rates | Higher success rates with medical supervision compared to self-detox. |
Explore related products






What You'll Learn
- Symptoms and Severity: Nausea, tremors, seizures, hallucinations, and delirium tremens (DTs) are common withdrawal symptoms
- Medical Detox Process: Medications like benzodiazepines, monitoring vitals, and IV fluids are used to manage withdrawal
- Duration of Stay: Hospitalization typically lasts 3-7 days, depending on symptom severity and complications
- Psychological Support: Counseling, therapy, and support groups are offered to address addiction and mental health
- Aftercare Planning: Discharge includes referrals to rehab, outpatient programs, and strategies to prevent relapse
![]()
Symptoms and Severity: Nausea, tremors, seizures, hallucinations, and delirium tremens (DTs) are common withdrawal symptoms
Alcohol withdrawal is a formidable adversary, and its symptoms can escalate rapidly from uncomfortable to life-threatening. Nausea often marks the beginning, a queasy reminder of the body’s struggle to recalibrate without alcohol. For those hospitalized, this is usually the first symptom addressed, as persistent vomiting can lead to dehydration and electrolyte imbalances, complicating recovery. Anti-nausea medications like ondansetron or intravenous fluids are commonly administered to stabilize patients, ensuring they can retain nutrients and medications essential for further treatment.
Tremors follow closely, a telltale sign of the nervous system’s agitation. These involuntary shakes, most noticeable in the hands, can begin within 6–48 hours after the last drink. In a hospital setting, tremors are monitored closely, as they often precede more severe symptoms. Benzodiazepines such as diazepam or lorazepam are frequently prescribed to dampen this overactivity, with dosages adjusted based on the patient’s age, weight, and severity of symptoms. For older adults or those with pre-existing health conditions, lower doses are typically initiated to avoid oversedation.
Seizures represent a critical juncture in alcohol withdrawal, occurring in about 3–5% of cases, often within 24–48 hours of cessation. These are not your typical seizures—they’re violent, unpredictable, and can cause injury if not managed promptly. Hospitalized patients are placed under continuous observation, and anti-seizure protocols are activated at the first sign of convulsions. Loading doses of benzodiazepines or anticonvulsants like carbamazepine may be administered, with the goal of preventing progression to the most feared complication: delirium tremens (DTs).
Hallucinations and DTs are the apex predators of alcohol withdrawal, striking fear into both patients and clinicians. Hallucinations, typically visual or auditory, can begin within 12–24 hours and are often the first sign of DTs, which affect 3–5% of withdrawing patients. DTs manifest as a terrifying triad: confusion, fever, and agitation, often accompanied by hallucinations. This condition is medical emergency, with a mortality rate of up to 15% if untreated. In the hospital, patients with DTs are transferred to intensive care units, where they receive high-dose benzodiazepines, antipsychotics, and sometimes barbiturates to sedate them into safety. Continuous cardiac monitoring and hydration are non-negotiable, as DTs can lead to heart arrhythmias and dehydration-induced kidney failure.
For those hospitalized, understanding the trajectory of these symptoms is both empowering and cautionary. Nausea and tremors are not merely inconveniences—they’re harbingers of what could come. Early intervention, often in the form of medication-assisted treatment and supportive care, can prevent the cascade into seizures, hallucinations, or DTs. Practical tips for patients include staying hydrated, avoiding triggers, and adhering strictly to prescribed regimens. For caregivers, vigilance is key: monitor for subtle changes in behavior or vital signs, as these can signal the onset of severe withdrawal. Alcohol withdrawal is a battle fought hour by hour, but with proper medical oversight, even the most severe symptoms can be managed, paving the way for recovery.
Hospitals: Profit-Driven Healthcare or Ethical Dilemma?
You may want to see also
Explore related products





![]()
Medical Detox Process: Medications like benzodiazepines, monitoring vitals, and IV fluids are used to manage withdrawal
Hospitalization for alcohol withdrawal is a critical intervention designed to manage the potentially life-threatening symptoms of detoxification. At its core, the medical detox process relies on a triad of interventions: medications like benzodiazepines, continuous monitoring of vital signs, and the administration of IV fluids. These measures work in tandem to stabilize the body, prevent complications, and ensure a safer transition to sobriety. Without such structured care, individuals face risks ranging from seizures to delirium tremens, a severe form of withdrawal that can be fatal.
Benzodiazepines, such as diazepam or lorazepam, are the cornerstone of pharmacological management during alcohol withdrawal. These medications act on the central nervous system to reduce hyperactivity caused by the absence of alcohol. Dosages are tailored to the severity of symptoms, often starting with 10–20 mg of diazepam every 1–2 hours until symptoms subside, then tapering over several days. For older adults or those with liver impairment, doses are typically reduced by 30–50% to minimize sedation and respiratory depression. It’s crucial to avoid abrupt discontinuation, as this can trigger rebound withdrawal. While benzodiazepines are effective, they are not without risks—dependence is a concern, making careful monitoring and gradual tapering essential.
Monitoring vitals is a non-negotiable aspect of inpatient detox. Nurses track heart rate, blood pressure, temperature, and respiratory rate every 4–6 hours, or more frequently if symptoms escalate. Elevated heart rate (tachycardia) and hypertension are early signs of withdrawal, while fever and irregular breathing may indicate progression to delirium tremens. Wearable monitors and continuous pulse oximetry are often employed to detect subtle changes. This vigilance allows medical staff to intervene promptly, adjusting medications or fluids as needed. For instance, a sudden spike in blood pressure might prompt an additional dose of a beta-blocker or a benzodiazepine to prevent seizures.
IV fluids play a dual role in alcohol withdrawal management: rehydration and electrolyte balance. Chronic alcohol use often leads to dehydration and deficiencies in magnesium, potassium, and thiamine. A standard regimen involves administering 1–2 liters of normal saline over 24 hours, supplemented with 20–40 mEq of potassium chloride and 2–4 grams of magnesium sulfate as needed. Thiamine, typically given as a 100 mg IV dose daily, prevents Wernicke’s encephalopathy, a neurological complication. IV access also ensures rapid delivery of emergency medications, such as lorazepam for seizures, which can be life-saving in acute situations.
The synergy of these interventions transforms a potentially chaotic and dangerous process into a controlled, therapeutic environment. Benzodiazepines calm the nervous system, vital sign monitoring provides early warning of complications, and IV fluids restore physiological balance. Together, they create a safety net that allows individuals to focus on the psychological and emotional aspects of recovery. While the process is rigorous, it is also deeply compassionate, recognizing that alcohol withdrawal is not just a physical challenge but a pivotal moment in reclaiming one’s health and future.
Butler, PA: Hospital Availability and Services
You may want to see also
Explore related products






![]()
Duration of Stay: Hospitalization typically lasts 3-7 days, depending on symptom severity and complications
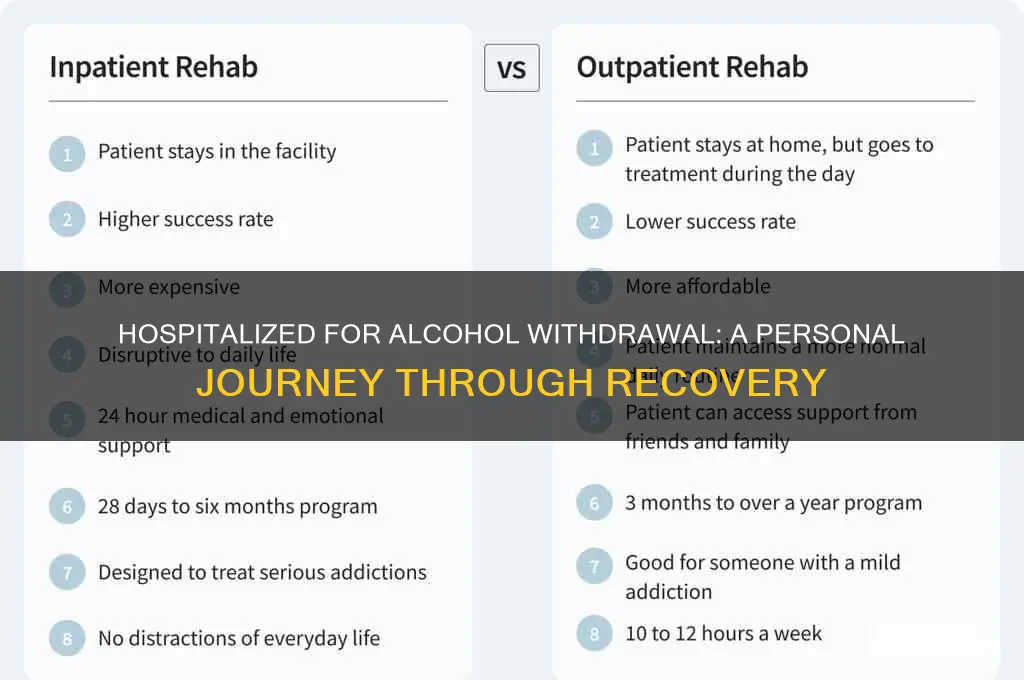
Hospital stays for alcohol withdrawal are often shorter than many expect, typically ranging from 3 to 7 days. This brevity might seem surprising given the complexity of withdrawal, but it’s a deliberate strategy. The goal is to stabilize the patient during the most acute phase, when symptoms like tremors, anxiety, and seizures peak. Beyond this window, ongoing care shifts to outpatient settings or specialized facilities, where long-term recovery strategies can be implemented.
The duration of hospitalization hinges on symptom severity and complications. Mild cases, characterized by symptoms like insomnia or nausea, may resolve within 3 days with medication and monitoring. Moderate cases, involving heightened anxiety or hallucinations, often require 5-7 days to manage safely. Severe cases, marked by delirium tremens (DTs), can extend the stay due to life-threatening risks like fever, seizures, or cardiovascular instability. For instance, a patient with DTs might receive benzodiazepines in escalating doses—starting at 20 mg of diazepam every hour—until symptoms subside, a process that can take several days.
Age and overall health play a critical role in determining length of stay. Younger, otherwise healthy individuals with no history of severe withdrawal may be discharged sooner, while older adults or those with comorbidities like liver disease often require extended monitoring. Practical tip: If you’re preparing for hospitalization, bring a list of all medications and pre-existing conditions to streamline the assessment process and potentially shorten your stay.
Comparatively, this 3-7 day window contrasts sharply with detox timelines for other substances. Opioid withdrawal, for example, often requires 5-10 days in a medical setting, while benzodiazepine withdrawal can span weeks due to tapering protocols. Alcohol withdrawal’s relatively short hospital stay underscores its unique challenges: rapid onset of symptoms and the need for immediate, intensive intervention.
Instructively, patients should understand that discharge doesn’t equate to full recovery. The hospital stay is a critical first step, but ongoing treatment—whether through therapy, support groups, or medication like naltrexone or acamprosate—is essential. A persuasive takeaway: View hospitalization as a lifeline, not the finish line. Use this brief but intense period to commit to a long-term recovery plan, leveraging the medical support and clarity gained during your stay.
Is Methodist Hospital San Antonio a Not-for-Profit Hospital?
You may want to see also
Explore related products





![]()
Psychological Support: Counseling, therapy, and support groups are offered to address addiction and mental health
Hospitalization for alcohol withdrawal often feels isolating, but psychological support is a cornerstone of recovery. Counseling, therapy, and support groups aren’t just add-ons—they’re essential tools to dismantle the mental grip of addiction. Unlike medication, which stabilizes the body, these interventions target the root causes of dependency, offering strategies to cope with triggers, rebuild self-worth, and envision a sober future. Without this dual approach, physical detoxification alone leaves patients vulnerable to relapse, as the psychological cravings and underlying issues remain unaddressed.
Consider the structure of therapy during hospitalization. Individual counseling sessions, typically 30–50 minutes long, focus on identifying patterns of behavior and thought that fuel addiction. Cognitive Behavioral Therapy (CBT), for instance, teaches patients to challenge distorted beliefs about alcohol, such as “I need it to relax” or “I can’t socialize without it.” Group therapy, often held daily in inpatient settings, fosters a sense of community and accountability. Here, patients share experiences, practice communication skills, and learn from peers who are navigating similar struggles. For those over 50, age-specific groups can address retirement-related triggers or health concerns that younger patients might not face.
Support groups like Alcoholics Anonymous (AA) or SMART Recovery are frequently introduced during hospitalization, providing a bridge to outpatient care. While some patients initially resist the idea of lifelong meetings, many find the 12-step model or self-empowerment frameworks invaluable. Practical tips for maximizing these groups include attending at least three meetings before deciding if it’s a fit, finding a sponsor within the first month, and actively participating rather than passively listening. For those wary of religious undertones in AA, secular alternatives like SMART Recovery focus on science-based techniques, such as cost-benefit analyses of drinking versus sobriety.
The role of family therapy cannot be overstated, especially for patients with codependent relationships or enabling behaviors at home. Sessions involving loved ones, typically 60–90 minutes, educate families about addiction as a disease, set boundaries, and rebuild trust. For adolescents (ages 13–17), involving parents or guardians is critical, as their support directly impacts treatment adherence. A key takeaway: psychological support isn’t just for the patient—it’s a family affair, reshaping dynamics to foster long-term recovery.
Finally, the integration of mental health treatment is vital, as over 50% of those with alcohol use disorder have co-occurring conditions like depression or anxiety. Hospital programs often include dual diagnosis therapy, where a single clinician addresses both addiction and mental health in coordinated sessions. Medication management, such as SSRIs for depression or naltrexone for cravings, may be paired with psychotherapy for a holistic approach. The goal isn’t just sobriety but emotional stability, equipping patients with tools to manage life’s stressors without reverting to alcohol. This comprehensive care transforms hospitalization from a crisis intervention into a launching pad for sustained wellness.
Training Employees: Two Point Hospital Style
You may want to see also
Explore related products






![]()
Aftercare Planning: Discharge includes referrals to rehab, outpatient programs, and strategies to prevent relapse
Hospitalization for alcohol withdrawal is often just the beginning of a long journey toward recovery. The physical stabilization achieved during this phase is crucial, but without a robust aftercare plan, the risk of relapse remains high. Discharge planning is not merely a formality; it’s a strategic bridge to sustained sobriety. Referrals to rehab, outpatient programs, and personalized relapse prevention strategies are the cornerstones of this process, each serving a distinct purpose in addressing the physical, psychological, and social dimensions of addiction.
Consider the case of a 45-year-old patient who completes a 5-day hospitalization for severe alcohol withdrawal, managed with benzodiazepines tapered over 72 hours. Upon discharge, a referral to a 28-day inpatient rehab program is made. This structured environment provides medical oversight, therapy, and peer support, critical for someone with a history of multiple relapses. In contrast, a 30-year-old with milder withdrawal symptoms might be better suited for an intensive outpatient program (IOP), which offers 9–12 hours of therapy weekly while allowing them to maintain work and family responsibilities. The choice between these options hinges on factors like the severity of addiction, social support, and the presence of co-occurring mental health disorders.
Outpatient programs, such as IOPs or standard outpatient therapy, are not one-size-fits-all. For instance, cognitive-behavioral therapy (CBT) sessions focus on identifying triggers and developing coping mechanisms, while medication-assisted treatment (MAT) with drugs like naltrexone or acamprosate can reduce cravings. A practical tip for patients in outpatient care is to create a daily schedule that includes therapy sessions, support group meetings (e.g., Alcoholics Anonymous), and healthy activities like exercise or hobbies. This structured routine minimizes idle time, a common relapse trigger.
Relapse prevention strategies must be tailored to individual needs. For someone whose drinking was tied to stress, mindfulness-based relapse prevention (MBRP) teaches techniques like meditation and breathwork to manage anxiety. For another whose social circle encourages drinking, building a sober support network through group therapy or community activities is essential. A key caution: avoiding high-risk situations, such as bars or events where alcohol is central, is non-negotiable in early recovery. Instead, patients should plan alternative activities, like joining a sports league or taking up a creative hobby.
The ultimate takeaway is that aftercare planning is not optional—it’s a lifeline. Without it, the 90% relapse rate within the first year of recovery becomes a looming threat. By combining professional treatment, structured programs, and proactive strategies, patients can navigate the challenges of sobriety with greater confidence. Discharge is not an endpoint but a transition, and the right aftercare plan ensures that the progress made in the hospital continues long after the patient leaves its walls.
Effective Hospital Fire Drill: Safety Steps and Staff Coordination Guide
You may want to see also
Frequently asked questions
Common symptoms include anxiety, tremors, sweating, nausea, insomnia, and in severe cases, seizures or hallucinations. Medical staff closely monitor these symptoms and provide medications like benzodiazepines to manage discomfort and prevent complications.
Hospitalization usually lasts 3 to 7 days, depending on the severity of withdrawal symptoms and individual health factors. Severe cases, such as those with delirium tremens (DTs), may require a longer stay for intensive care and monitoring.
Patients receive medical supervision, medications to ease symptoms, and intravenous fluids to address dehydration or electrolyte imbalances. Additionally, counseling or referrals to addiction specialists are often provided to support long-term recovery and prevent relapse.