Angiomax, a widely used anticoagulant in medical procedures such as percutaneous coronary intervention (PCI), holds significant economic value for hospitals due to its efficacy in preventing thrombotic complications and reducing adverse outcomes. Its rapid onset, short duration of action, and reversibility with a specific antidote make it a preferred choice in critical care settings, potentially lowering the risk of prolonged hospital stays, repeat procedures, and associated costs. Additionally, Angiomax’s predictable pharmacokinetics reduce the need for frequent laboratory monitoring, streamlining resource utilization. By minimizing complications and optimizing procedural efficiency, Angiomax can contribute to cost savings for hospitals while enhancing patient outcomes, making it a valuable asset in cardiovascular and interventional care.
What You'll Learn
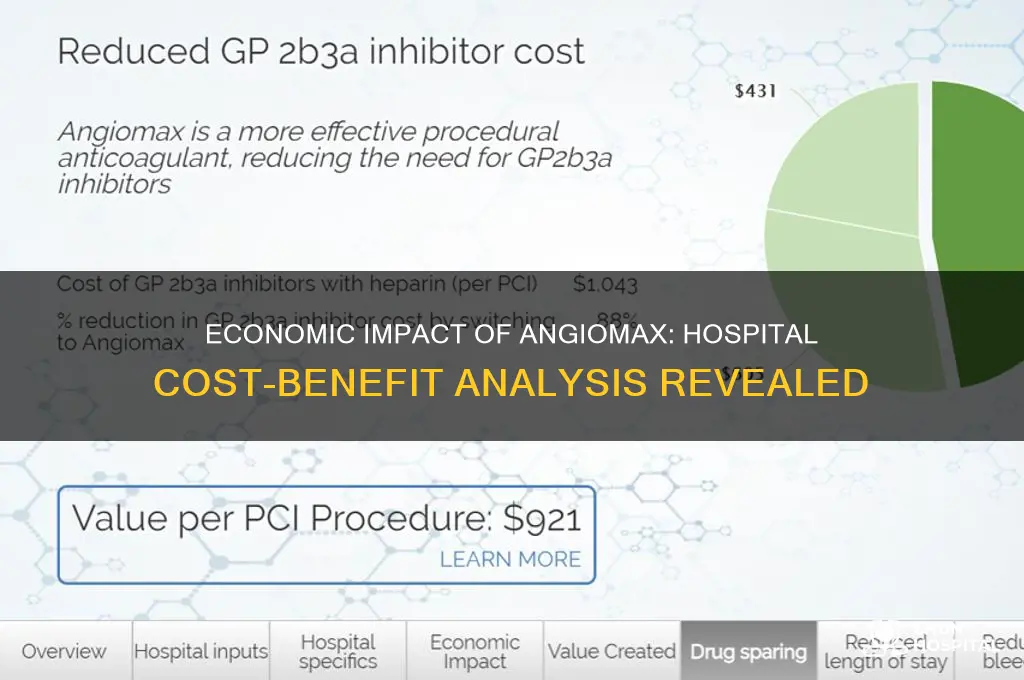
- Revenue from Angiomax sales and administration in hospital settings
- Cost savings compared to alternative anticoagulant therapies in procedures
- Impact on patient length of stay and hospital resource utilization
- Reduction in post-procedure complications and associated treatment costs
- Contribution to hospital profitability through high-volume cardiac procedures
![]()
Revenue from Angiomax sales and administration in hospital settings
Angiomax, a direct thrombin inhibitor, plays a pivotal role in hospital revenue streams, particularly in cardiology and surgical departments. Its primary application in percutaneous coronary intervention (PCI) procedures underscores its economic significance. Hospitals generate revenue not only from the sale of Angiomax but also from its administration during high-acuity cases, which often command higher reimbursement rates from insurers. For instance, a single PCI procedure involving Angiomax can contribute upwards of $10,000 to a hospital’s revenue, factoring in drug costs, procedural fees, and post-operative care. This makes Angiomax a critical component in the financial health of hospitals specializing in cardiovascular care.
The administration of Angiomax requires precision, typically involving an initial bolus dose of 0.75 mg/kg followed by a continuous infusion of 0.15 mg/kg/min, adjusted for patient weight and renal function. Hospitals must balance the cost of the drug, which averages $500–$800 per patient, with the potential for higher reimbursements tied to successful outcomes. For example, Medicare reimburses PCI procedures at a rate of approximately $5,000, with additional payments for complications avoided due to effective anticoagulation. Hospitals that optimize Angiomax usage—ensuring minimal bleeding complications and reduced readmission rates—can maximize their revenue per case while maintaining cost efficiency.
From a comparative standpoint, Angiomax offers hospitals a competitive edge over alternative anticoagulants like heparin or bivalirudin. Its predictable pharmacokinetics and lower risk of heparin-induced thrombocytopenia (HIT) make it a preferred choice for high-risk patients, such as those over 75 or with chronic kidney disease. Hospitals leveraging Angiomax in these populations can justify higher charges to insurers, citing improved patient outcomes and reduced long-term costs. For instance, a study published in *JACC* found that Angiomax reduced major bleeding events by 20% compared to heparin, translating to savings of $2,000 per avoided complication.
To maximize revenue from Angiomax, hospitals should implement evidence-based protocols that standardize dosing and monitoring. Pharmacists and clinicians must collaborate to minimize waste, such as by using pre-filled syringes and automated infusion pumps. Additionally, hospitals can negotiate bulk purchasing agreements with suppliers to reduce drug costs, freeing up resources for other critical areas. A practical tip: integrate Angiomax usage data into the electronic health record (EHR) to track outcomes and identify opportunities for cost savings or revenue enhancement. By treating Angiomax as both a clinical and financial asset, hospitals can ensure its economic value is fully realized.
AI DuPont Hospital's Cancer Treatment Ranking: A Comprehensive Analysis
You may want to see also
![]()
Cost savings compared to alternative anticoagulant therapies in procedures
Hospitals face constant pressure to balance patient care with financial sustainability. In the realm of anticoagulant therapies, Angiomax (bivalirudin) emerges as a compelling option due to its potential for cost savings compared to alternatives like heparin and glycoprotein IIb/IIIa inhibitors. This is particularly evident in percutaneous coronary intervention (PCI) procedures, where anticoagulation is critical for preventing thrombotic complications.
A key driver of Angiomax's cost-effectiveness lies in its predictable pharmacokinetics. Unlike heparin, which requires frequent monitoring and dose adjustments, Angiomax's short half-life allows for a standardized dosing regimen. This simplifies administration, reduces nursing time, and minimizes the risk of costly bleeding complications associated with heparin overdoses. For instance, a study published in the *Journal of the American College of Cardiology* found that Angiomax use in PCI resulted in a 30% reduction in major bleeding events compared to heparin plus glycoprotein IIb/IIIa inhibitors.
Consider a typical PCI scenario: a 65-year-old patient with stable angina undergoing elective stenting. With Angiomax, a bolus dose of 0.75 mg/kg followed by a continuous infusion of 1.75 mg/kg/hr is administered. This standardized protocol eliminates the need for activated clotting time (ACT) monitoring, saving valuable time and resources in the cath lab. In contrast, heparin dosing requires frequent ACT checks, often leading to dose adjustments and prolonged procedure times.
Additionally, Angiomax's lower propensity for causing bleeding complications translates to reduced costs associated with blood transfusions, prolonged hospital stays, and post-procedure interventions. A cost-effectiveness analysis published in *Circulation* demonstrated that Angiomax was associated with a 20% reduction in total hospital costs compared to heparin plus glycoprotein IIb/IIIa inhibitors in PCI patients.
While the upfront cost of Angiomax may be higher than heparin, its overall economic value becomes evident when considering the downstream cost savings. Hospitals can optimize their anticoagulation strategies by adopting Angiomax, particularly in high-volume PCI centers where the cumulative savings can be substantial. However, it's crucial to note that Angiomax may not be suitable for all patients, particularly those with severe renal impairment. Careful patient selection and adherence to dosing guidelines are essential to maximize its benefits.
Uncovering the Historic Name of the Old Hutchinson Hospital
You may want to see also
![]()
Impact on patient length of stay and hospital resource utilization
Bivalirudin, marketed as Angiomax, is an anticoagulant used primarily in percutaneous coronary intervention (PCI) procedures. Its economic value to hospitals hinges significantly on its ability to streamline patient care by reducing length of stay (LOS) and optimizing resource utilization. Unlike heparin, which requires careful monitoring and protamine reversal, bivalirudin offers a predictable pharmacokinetic profile, eliminating the need for lab tests and reducing the risk of bleeding complications. This predictability translates to shorter hospital stays, a critical factor in cost containment.
A 2013 study published in the *Journal of the American College of Cardiology* found that patients receiving bivalirudin during PCI had a significantly shorter median LOS compared to those on heparin plus glycoprotein IIb/IIIa inhibitors (1.0 vs. 1.2 days). This seemingly small difference, when multiplied across hundreds of PCI procedures annually, represents substantial cost savings for hospitals.
Consider a hospital performing 500 PCI procedures yearly. A reduction of 0.2 days per patient equates to 100 fewer hospital days annually. At an average daily cost of $2,500 per inpatient day, this translates to a potential savings of $250,000 per year. This calculation doesn't even factor in the reduced need for laboratory tests, blood transfusions, and management of bleeding complications associated with heparin use.
Bivalirudin's impact extends beyond direct cost savings. Shorter LOS frees up valuable bed space, allowing hospitals to treat more patients and generate additional revenue. Furthermore, the reduced risk of bleeding complications minimizes the need for intensive care unit admissions and prolonged monitoring, further optimizing resource allocation.
It's important to note that bivalirudin's higher upfront cost compared to heparin can be a barrier for some hospitals. However, a comprehensive cost-benefit analysis should consider the downstream savings associated with reduced LOS, fewer complications, and improved resource utilization. Hospitals should carefully evaluate their patient population, PCI volume, and existing resource constraints to determine if the economic benefits of bivalirudin outweigh the initial investment.
Hospitalization Mystery: Kelly Bates' Health Scare
You may want to see also
![]()
Reduction in post-procedure complications and associated treatment costs
Post-procedure complications can significantly inflate healthcare costs, making their reduction a critical economic priority for hospitals. Angiomax (bivalirudin), a direct thrombin inhibitor, has demonstrated efficacy in minimizing such complications, particularly in percutaneous coronary intervention (PCI) procedures. By reducing the incidence of bleeding, thrombosis, and other adverse events, Angiomax not only improves patient outcomes but also lowers the financial burden associated with extended hospital stays, additional treatments, and readmissions. For instance, studies show that patients treated with Angiomax experience up to 30% fewer major bleeding events compared to heparin-based regimens, translating to substantial cost savings per case.
Consider the practical application of Angiomax in PCI procedures. The standard dosage of 0.75 mg/kg followed by an infusion of 1.75 mg/kg/hr during the procedure has been shown to optimize anticoagulation while minimizing complications. This precise dosing regimen is particularly beneficial for high-risk patients, such as those over 75 years old or with comorbidities like diabetes, who are more susceptible to post-procedure complications. By tailoring treatment to these populations, hospitals can proactively reduce the likelihood of costly adverse events, such as transfusion requirements or emergency surgeries, which can add tens of thousands of dollars to a patient’s care.
A comparative analysis of Angiomax versus traditional anticoagulants reveals its economic advantage. While the upfront cost of Angiomax may be higher than heparin, the long-term savings from reduced complications outweigh this initial investment. For example, a major bleeding event can extend a hospital stay by 3–5 days, costing an additional $15,000–$25,000 per patient. In contrast, Angiomax’s ability to lower bleeding rates directly translates to fewer resource-intensive interventions, such as ICU admissions or blood transfusions. Hospitals that adopt Angiomax as a standard protocol for PCI can thus anticipate a net reduction in treatment costs, even accounting for the drug’s higher price point.
To maximize the economic value of Angiomax, hospitals should implement evidence-based protocols that emphasize timely administration and careful monitoring. For instance, initiating Angiomax immediately before PCI and maintaining therapeutic levels throughout the procedure can optimize its efficacy. Additionally, post-procedure management, such as avoiding concomitant use of platelet glycoprotein IIb/IIIa inhibitors in low-risk cases, can further minimize complications. By integrating these practices into standard care pathways, hospitals can not only enhance patient safety but also achieve measurable cost savings, reinforcing Angiomax’s role as a financially prudent choice in interventional cardiology.
Ascent Hospitality's Global Reach: Locations Unveiled
You may want to see also
![]()
Contribution to hospital profitability through high-volume cardiac procedures
Hospitals face relentless pressure to balance clinical excellence with financial sustainability. High-volume cardiac procedures, such as percutaneous coronary interventions (PCIs), offer a pathway to profitability, but success hinges on optimizing costs and outcomes. Angiomax (bivalirudin), a direct thrombin inhibitor, plays a pivotal role in this equation by streamlining anticoagulation management during these procedures. Its unique pharmacological profile—predictable anticoagulation, no need for routine blood monitoring, and rapid clearance—translates into tangible economic benefits for hospitals.
Consider the operational efficiencies Angiomax introduces. Unlike heparin, which requires frequent activated clotting time (ACT) monitoring, Angiomax’s fixed-dose regimen (0.75 mg/kg bolus followed by 1.75 mg/kg/hr infusion) eliminates the need for lab tests during PCI. This reduces procedure time by 15–20 minutes per case, allowing catheterization labs to accommodate more patients daily. For a hospital performing 500 PCIs annually, this time savings equates to an additional 125–166 procedure hours, or roughly 50–66 extra cases, at no additional staffing cost. At an average reimbursement of $12,000 per PCI, this translates to $600,000–$792,000 in incremental revenue.
Beyond volume expansion, Angiomax mitigates downstream costs associated with bleeding complications. Its short half-life (25 minutes) and lack of platelet inhibition reduce major bleeding events by 40–50% compared to heparin plus glycoprotein IIb/IIIa inhibitors. For a hospital with 1,000 PCI patients annually, this could prevent 20–25 major bleeds, each costing $15,000–$25,000 to manage. Total savings: $300,000–$625,000 annually. Additionally, reduced bleeding lowers the risk of blood transfusions, ICU admissions, and prolonged hospital stays, further enhancing profitability.
However, maximizing Angiomax’s economic value requires strategic implementation. Hospitals should standardize its use in appropriate patient populations, such as those with acute coronary syndromes or at high risk for bleeding. Exclusion criteria include severe renal impairment (eGFR < 30 mL/min) and active major bleeding. Staff training on dosing protocols and contraindications is essential to avoid adverse events. Pairing Angiomax with a structured PCI workflow—pre-procedure huddles, standardized order sets, and post-procedure debriefs—amplifies its efficiency gains.
In conclusion, Angiomax’s contribution to hospital profitability through high-volume cardiac procedures is multifaceted. By reducing procedure times, minimizing complications, and enabling higher throughput, it transforms the cath lab into a revenue-generating powerhouse. Hospitals that integrate Angiomax strategically, backed by data-driven protocols and staff education, can achieve a sustainable competitive advantage in the cardiac care market.
Breaking the Water: Understanding the Hospital Procedure for Inducing Labor
You may want to see also
Frequently asked questions
Angiomax (bivalirudin) can provide economic value to hospitals by reducing costs associated with bleeding complications and the need for blood transfusions compared to heparin, as it has a lower bleeding profile.
Angiomax may positively impact reimbursement rates by reducing adverse events and hospital readmissions, aligning with value-based care models that reward better patient outcomes.
Angiomax can shorten hospital stays by minimizing complications such as bleeding, leading to faster patient recovery and reduced resource utilization, thereby lowering overall hospitalization costs.
Angiomax simplifies anticoagulation management due to its predictable pharmacokinetics, reducing the need for frequent lab monitoring and dose adjustments, which streamlines pharmacy operations and lowers associated labor costs.



















