Escherichia coli (E. coli), commonly found in the human gut, can cause a range of infections in hospital settings, particularly in immunocompromised patients or those with invasive medical devices. In hospitals, E. coli is a leading cause of urinary tract infections (UTIs), often associated with catheter use, as well as bloodstream infections (bacteremia or sepsis), which can be life-threatening. Additionally, it may cause pneumonia, especially in ventilated patients, and surgical site or wound infections. Certain pathogenic strains, such as Shiga-toxin-producing E. coli (STEC), can also lead to gastrointestinal infections, though these are less common in hospital environments. The prevalence of antibiotic-resistant E. coli strains in healthcare facilities further complicates treatment, making it a significant concern for infection control and patient safety.
| Characteristics | Values |
|---|---|
| Types of Infections | Urinary Tract Infections (UTIs), bloodstream infections (bacteremia/sepsis), pneumonia, surgical site infections, meningitis (in neonates), and intra-abdominal infections. |
| Common Sites | Urinary tract, bloodstream, respiratory tract, surgical wounds, central nervous system (neonates), and abdominal cavity. |
| Risk Factors | Prolonged hospital stays, invasive procedures (e.g., catheter use), weakened immune systems, and antibiotic exposure. |
| Transmission | Person-to-person contact, contaminated medical equipment, or environmental surfaces. |
| Antibiotic Resistance | Increasing prevalence of multidrug-resistant (MDR) and extended-spectrum beta-lactamase (ESBL)-producing strains. |
| Prevention Measures | Hand hygiene, proper sterilization of equipment, prudent antibiotic use, and infection control protocols. |
| Mortality Rate | Varies; bloodstream infections (sepsis) have higher mortality, especially in immunocompromised patients. |
| Common Strains | E. coli ST131, ESBL-producing strains, and carbapenem-resistant E. coli. |
| Symptoms | Fever, chills, pain at infection site, confusion (in severe cases), and organ dysfunction (sepsis). |
| Diagnosis | Blood cultures, urine cultures, imaging, and antimicrobial susceptibility testing. |
| Treatment | Antibiotics (e.g., carbapenems, fosfomycin) based on susceptibility; supportive care for severe cases. |
| Global Burden | Leading cause of healthcare-associated infections (HAIs), particularly in intensive care units (ICUs). |
Explore related products




What You'll Learn
- Urinary Tract Infections (UTIs): E. coli is the leading cause of hospital-acquired UTIs
- Bloodstream Infections (Bacteremia): E. coli can enter the bloodstream, causing sepsis
- Pneumonia: Hospitalized patients, especially on ventilators, risk E. coli lung infections
- Surgical Site Infections: E. coli can infect wounds post-surgery, delaying healing
- Meningitis: Rare but severe, E. coli can cause brain and spinal cord infections
![]()
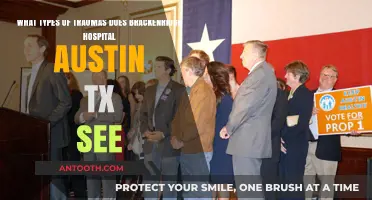
Urinary Tract Infections (UTIs): E. coli is the leading cause of hospital-acquired UTIs
E. coli, a bacterium commonly found in the human gut, is a notorious culprit in hospital-acquired infections, particularly urinary tract infections (UTIs). These infections are a significant concern in healthcare settings, affecting up to 10% of patients during their hospital stay. The risk is especially high among those with urinary catheters, where E. coli can easily ascend from the urethra to the bladder, causing cystitis, or further to the kidneys, leading to pyelonephritis. This bacterium's ability to form biofilms on catheter surfaces makes it a persistent and challenging pathogen to eradicate.
Understanding the Risk Factors
Hospitalized patients face heightened UTI risks due to invasive procedures, prolonged catheter use, and compromised immune systems. E. coli accounts for approximately 80% of catheter-associated UTIs, thriving in the stagnant urine environment. Other risk factors include female anatomy, advanced age, diabetes, and recent antibiotic use, which can disrupt normal flora and allow E. coli to dominate. Recognizing symptoms early—such as fever, flank pain, or cloudy urine—is crucial, though many hospital-acquired UTIs are asymptomatic, detected only through routine screening.
Prevention Strategies in Clinical Settings
Hospitals employ evidence-based practices to reduce E. coli-related UTIs. These include minimizing catheter use, ensuring proper insertion and maintenance, and using antimicrobial-coated catheters. Healthcare providers are trained to follow strict aseptic techniques, such as hand hygiene and sterile equipment handling. For high-risk patients, probiotics or targeted antibiotics may be considered, though overuse is avoided to prevent antibiotic resistance. Patient education on hydration and hygiene also plays a role in prevention.
Treatment Approaches and Challenges
When E. coli UTIs occur, treatment typically involves empiric antibiotics like nitrofurantoin, trimethoprim-sulfamethoxazole, or fosfomycin, with dosages adjusted for age and renal function (e.g., 100 mg nitrofurantoin twice daily for 5 days in adults). However, rising antibiotic resistance complicates therapy, with some E. coli strains exhibiting resistance to first-line agents. Culture and sensitivity testing are essential to guide treatment, and alternative options like ceftriaxone or ampicillin may be required. In severe cases, intravenous antibiotics and extended treatment durations are necessary to prevent complications like sepsis.
Long-Term Implications and Patient Outcomes
Hospital-acquired E. coli UTIs not only prolong hospital stays but also increase healthcare costs and mortality rates, particularly in elderly or immunocompromised patients. Recurrent infections can lead to chronic kidney damage or urosepsis, emphasizing the need for proactive management. Hospitals must balance infection control measures with judicious antibiotic use to curb resistance. For patients, understanding their risk and advocating for timely catheter removal or alternative interventions can significantly improve outcomes.
Exploring the Massive LEGO Hospital Set
You may want to see also
Explore related products






![]()
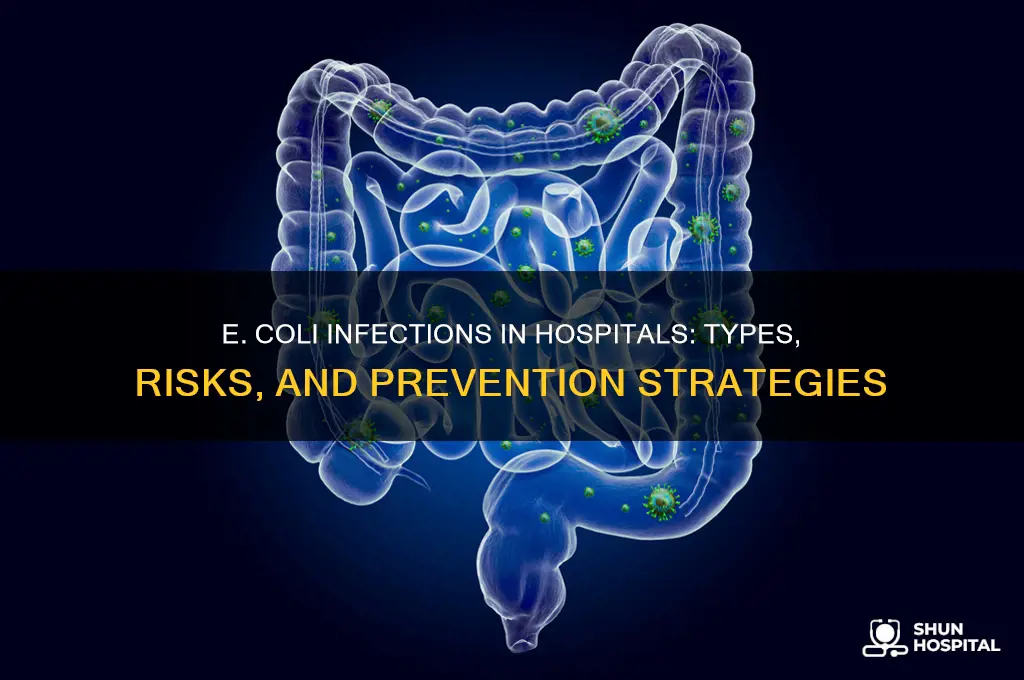
Bloodstream Infections (Bacteremia): E. coli can enter the bloodstream, causing sepsis
E. coli bloodstream infections, or bacteremia, represent a critical concern in hospital settings, often escalating to life-threatening sepsis. This occurs when E. coli, typically a gut bacterium, breaches the intestinal barrier or enters via medical procedures, gaining access to the bloodstream. Once there, it triggers a systemic immune response, leading to widespread inflammation and organ dysfunction. Patients with weakened immune systems, those undergoing invasive procedures, or individuals with indwelling catheters are particularly vulnerable. Recognizing the early signs—fever, chills, rapid heartbeat, and confusion—is crucial for prompt intervention.
The progression from bacteremia to sepsis is rapid and requires immediate medical attention. Sepsis is a medical emergency characterized by a severe imbalance in the body’s response to infection, often resulting in shock, organ failure, or death. Hospitals employ aggressive treatment protocols, including broad-spectrum antibiotics administered intravenously within the first hour of recognition, a practice known as the "sepsis bundle." Empiric therapy often includes combinations like piperacillin-tazobactam (4.5 g every 6 hours) or cefepime (2 g every 8 hours), tailored later based on antibiotic susceptibility testing. Delayed treatment increases mortality risk, emphasizing the need for swift action.
Comparatively, E. coli bloodstream infections differ from other hospital-acquired infections due to their propensity to cause systemic complications. While urinary tract infections (UTIs) or surgical site infections may remain localized, bacteremia bypasses these barriers, directly challenging the body’s core systems. This distinction underscores the importance of preventive measures, such as strict hand hygiene, sterile techniques during procedures, and judicious use of antibiotics to avoid resistance. Hospitals must also monitor high-risk patients closely, particularly those in intensive care units or with prolonged hospital stays.
Practically, healthcare providers can mitigate risks by adhering to evidence-based guidelines. For instance, removing unnecessary catheters, using chlorhexidine for skin antisepsis, and implementing bundled care protocols significantly reduce infection rates. Patients and families should be educated on recognizing early symptoms and advocating for timely testing, such as blood cultures, which confirm E. coli as the causative agent. While hospitals are inherently high-risk environments, proactive strategies can curb the incidence and severity of E. coli bloodstream infections, saving lives and reducing healthcare burdens.
Ambetter Insurance: Northside Hospital In-Network?
You may want to see also
Explore related products






![]()
Pneumonia: Hospitalized patients, especially on ventilators, risk E. coli lung infections
Hospitalized patients, particularly those on ventilators, face a heightened risk of developing E. coli-induced pneumonia, a severe and often overlooked complication. This occurs when the bacterium, typically associated with gastrointestinal infections, migrates to the lungs, exploiting the compromised respiratory defenses of vulnerable patients. Ventilators, while life-saving, create a direct pathway for pathogens to enter the lower respiratory tract, bypassing natural filters like the mouth and throat. Studies show that up to 20% of ventilator-associated pneumonias (VAP) are caused by Gram-negative bacteria, including *E. coli*, particularly in intensive care units (ICUs).
The mechanism behind this infection is twofold. First, intubation disrupts the cough reflex and mucociliary clearance, allowing bacteria to accumulate in the lungs. Second, *E. coli* strains in hospitals often exhibit multidrug resistance (MDR), making treatment challenging. For instance, extended-spectrum beta-lactamase (ESBL)-producing *E. coli* is increasingly reported in VAP cases, requiring empiric therapy with carbapenems or alternative agents like tigecycline. Early identification of risk factors—such as prolonged ventilation, prior antibiotic use, and immunosuppression—is critical for prevention.
Preventive measures are multifaceted. Healthcare providers must adhere to strict hand hygiene protocols and ventilator bundle care, including elevating the head of the bed to 30–45 degrees and daily sedation vacations to assess weaning potential. Patients should receive oral care with chlorhexidine gluconate (0.12% solution) every 6 hours to reduce oral bacterial colonization. For high-risk individuals, selective digestive decontamination (SDD) with topical antibiotics may be considered, though its use remains controversial due to concerns about fostering resistance.
Clinicians must remain vigilant for signs of *E. coli* pneumonia, which include fever, purulent sputum, and worsening oxygenation. Diagnosis relies on clinical suspicion, chest imaging, and microbiological confirmation via bronchoalveolar lavage or endotracheal aspirates. Treatment involves broad-spectrum antibiotics tailored to susceptibility testing, with combination therapy (e.g., piperacillin-tazobactam plus an aminoglycoside) reserved for severe cases. Prompt de-escalation is essential to minimize resistance and adverse effects.
In conclusion, *E. coli* pneumonia in hospitalized patients, especially those on ventilators, represents a critical intersection of infection control and antimicrobial stewardship. By understanding the unique vulnerabilities of this population and implementing evidence-based interventions, healthcare teams can mitigate the risk of this life-threatening complication. Proactive surveillance, judicious antibiotic use, and adherence to best practices in ventilator care are paramount to protecting patients from this insidious threat.
Sibley Hospital Location: A Guide to Finding It in Washington DC
You may want to see also
Explore related products





![]()
Surgical Site Infections: E. coli can infect wounds post-surgery, delaying healing
E. coli, often associated with foodborne illnesses, is a formidable pathogen in hospital settings, particularly when it infiltrates surgical wounds. Postoperative surgical site infections (SSIs) caused by *E. coli* are a significant concern, as they can substantially delay healing, prolong hospital stays, and increase the risk of complications. These infections typically occur within 30 days of surgery, manifesting as redness, swelling, pus, or pain around the incision site. The bacterium can enter the wound during surgery or through postoperative contamination, exploiting the body’s weakened state to establish infection.
The risk of *E. coli*-induced SSIs is higher in abdominal surgeries, such as appendectomies or colorectal procedures, due to the bacterium’s natural presence in the gastrointestinal tract. Patients with compromised immune systems, diabetes, or those undergoing prolonged procedures are particularly vulnerable. Preventive measures include strict aseptic techniques during surgery, prophylactic antibiotics administered within 60 minutes before incision (e.g., cefazolin 1–2 g IV), and meticulous wound care post-operation. Healthcare providers must also educate patients on keeping the surgical site clean and dry, recognizing early signs of infection, and seeking prompt medical attention if symptoms arise.
Comparatively, *E. coli* SSIs differ from other wound infections in their rapid progression and resistance potential. Unlike infections caused by *Staphylococcus aureus*, *E. coli* often responds to first-line antibiotics like cephalosporins or fluoroquinolones, but increasing antibiotic resistance underscores the need for judicious use. Hospitals should implement surveillance programs to monitor *E. coli* strains and tailor treatment protocols accordingly. For instance, if a strain exhibits resistance to ampicillin, alternative agents like piperacillin-tazobactam or carbapenems may be necessary.
From a practical standpoint, patients can reduce their risk by adhering to preoperative instructions, such as showering with chlorhexidine soap the night before surgery and avoiding shaving the surgical area themselves, as this can cause micro-abrasions that invite bacterial entry. Postoperatively, elevating the wound (when applicable) and changing dressings regularly can minimize infection risk. Hospitals should also optimize operating room conditions, maintaining humidity below 60% and temperature between 20–24°C to reduce bacterial proliferation. By combining patient education, rigorous protocols, and targeted treatment, healthcare teams can mitigate the impact of *E. coli* on surgical site healing and improve patient outcomes.
The Rural Hospital Crisis in Georgia: Why Did They Close?
You may want to see also
Explore related products

$26.99


![]()
Meningitis: Rare but severe, E. coli can cause brain and spinal cord infections
E. coli, often associated with gastrointestinal infections, can also cause rare but severe cases of meningitis, particularly in neonates and young infants. This form of meningitis occurs when the bacterium invades the bloodstream and crosses the blood-brain barrier, leading to inflammation of the protective membranes surrounding the brain and spinal cord. Neonatal E. coli meningitis is a medical emergency, with symptoms including fever, irritability, poor feeding, and bulging fontanelles. Immediate diagnosis and treatment are critical, as delays can result in long-term neurological damage or death.
The pathophysiology of E. coli meningitis involves the bacterium's ability to evade the immune system and adhere to endothelial cells. Strains producing K1 capsule, a polysaccharide antigen, are particularly virulent due to their ability to mimic human brain tissue, avoiding phagocytosis. This mechanism underscores the bacterium's adaptability and the challenges in treating such infections. Antibiotic therapy, typically involving a combination of third-generation cephalosporins like cefotaxime (50 mg/kg every 6 hours) and ampicillin (200 mg/kg/day), is standard. However, increasing antibiotic resistance necessitates susceptibility testing to guide treatment.
Comparatively, E. coli meningitis differs from other bacterial causes, such as Streptococcus pneumoniae or Neisseria meningitidis, in its prevalence and risk factors. While pneumococcal and meningococcal meningitis are more common in older children and adults, E. coli meningitis predominantly affects newborns, particularly those born preterm or with low birth weight. This highlights the importance of targeted preventive measures, such as maternal screening for E. coli colonization during pregnancy and strict hygiene practices in neonatal units.
Practically, healthcare providers must remain vigilant for signs of sepsis in neonates, as E. coli meningitis often presents as a complication of bacteremia. Early recognition involves monitoring for subtle symptoms like lethargy or respiratory distress, which may precede the classic signs of meningitis. Parents and caregivers should be educated on seeking immediate medical attention for any concerning symptoms in infants, especially those at higher risk. Additionally, hospitals should implement infection control protocols, including hand hygiene and environmental disinfection, to minimize the spread of E. coli in neonatal wards.
In conclusion, while E. coli meningitis is rare, its severity demands proactive management. Understanding the bacterium's virulence factors, recognizing high-risk populations, and adhering to evidence-based treatment protocols are essential for improving outcomes. By combining clinical vigilance with preventive strategies, healthcare systems can mitigate the impact of this life-threatening infection on vulnerable neonates.
US Hospital Computers: Down and Out?
You may want to see also
Frequently asked questions
E. coli in hospitals commonly causes urinary tract infections (UTIs), bloodstream infections (bacteremia/sepsis), pneumonia, and surgical site infections. These infections often occur in immunocompromised or hospitalized patients.
Yes, E. coli can cause gastrointestinal infections in hospitals, particularly in outbreaks linked to contaminated food, water, or poor hygiene. However, these are less common in hospital settings compared to community outbreaks.
Yes, E. coli can cause wound and surgical site infections, especially in patients with prolonged hospital stays, invasive procedures, or weakened immune systems. Proper wound care and infection control measures are critical to prevention.
Yes, E. coli is a leading cause of bloodstream infections (sepsis) in hospitals, particularly in intensive care units (ICUs) and among patients with indwelling devices like catheters. These infections are serious and require prompt antibiotic treatment.