Diabetic ketoacidosis (DKA) is a serious, life-threatening condition that requires urgent treatment in a hospital. It is characterized by hyperglycemia, acidosis, and ketonemia and is usually observed in patients with type 1 diabetes, although it can also occur in those with type 2 diabetes. The treatment of DKA in a hospital setting involves initial rehydration with isotonic saline, followed by potassium replacement and low-dose insulin therapy. Intravenous fluids and electrolytes are administered to replace losses and regulate blood sugar levels. Close monitoring is required to prevent and manage potential complications affecting the brain, heart, or lungs. The resolution of DKA can take several hours, and patients are typically discharged once they can manage their insulin regimen without a recurrence of ketosis.
| Characteristics | Values |
|---|---|
| Treatment Location | Intensive care unit, step-down unit, general medical ward, or emergency department |
| Treatment Time | First 24-48 hours |
| Treatment Type | Insulin therapy, fluid replacement, electrolyte replacement, glucose monitoring, rehydration, potassium replacement, low-dose insulin therapy |
| Patient Monitoring | Vigilance for concomitant processes such as infection, cerebrovascular accident, myocardial infarction, sepsis, or deep venous thrombosis |
| Discharge Criteria | Return to daily insulin regimen without recurrence of ketosis |
| Patient Population | Commonly patients with type 1 diabetes, but also occurs in patients with type 2 diabetes |
| Precipitating Factors | Non-compliance, new-onset diabetes, acute medical illness, trauma, surgery, infections, period, not taking enough insulin |
| Mortality Rate | Less than 5% with standardized treatment guidelines |
Explore related products






What You'll Learn
- Monitor for concomitant processes like infection, myocardial infarction, or sepsis
- Administer fluids to correct fluid loss and thin out blood sugar
- Provide electrolyte replacement to maintain heart, muscle, and nerve cell function
- Administer insulin therapy to reverse diabetic ketoacidosis
- Discharge patients when they can resume their daily insulin regimen
![]()
Monitor for concomitant processes like infection, myocardial infarction, or sepsis
Diabetic ketoacidosis (DKA) is a life-threatening complication of diabetes that requires immediate treatment. It is characterized by hyperglycemia, acidosis, and ketonemia. Patients with DKA are typically admitted to the intensive care unit for the first 24-48 hours of treatment. During this critical period, it is essential to monitor for any concomitant processes, including infection, myocardial infarction, sepsis, cerebrovascular accident, or deep venous thrombosis.
Infection and sepsis are common triggers of DKA, particularly in patients with type 1 diabetes. Pneumonia and urinary tract infections are the most prevalent types of infections associated with DKA. Therefore, when treating DKA, it is crucial to be vigilant for signs and symptoms of infection and to initiate proper antibiotic therapy if necessary. Culture and sensitivity studies guide the selection of antibiotics, but empiric antibiotics may be started if infection is suspected while awaiting culture results.
Myocardial infarction (MI) is another concomitant process to monitor for in patients with DKA. Nonspecific myocardial injury can occur in severe DKA, with minor elevations in myocardial biomarkers (troponin T and CK-MB) and ECG changes that may indicate MI. However, these elevations and ECG changes do not necessarily confirm MI in the context of DKA. The mechanisms responsible for DKA and myocardial infarction with nonobstructive coronary arteries (MINOCA) overlap, and a decompensated hyperglycemic state can produce MI without epicardial coronary obstruction.
Additionally, it is important to correct fluid and electrolyte loss during the first hour of treatment for DKA. This is followed by a gradual correction of hyperglycemia and acidosis. Dehydration, even in its mild forms, is an indicator that the patient has already lost at least 3 litres of fluid. Intravenous (IV) fluids are often used to correct fluid loss, and IV electrolytes are administered to maintain the proper functioning of the heart, muscles, and nerve cells.
Charing Cross Hospital: Congestion Zone Charges?
You may want to see also
Explore related products






![]()
Administer fluids to correct fluid loss and thin out blood sugar
Diabetic ketoacidosis (DKA) is a life-threatening complication of diabetes. It is characterized by hyperglycemia, acidosis, and ketonemia. The treatment of DKA in a hospital setting involves several steps, including fluid administration, electrolyte replacement, and insulin therapy.
Administering fluids is a crucial aspect of treating DKA. Fluids are given to replace those lost through frequent urination, a common symptom of DKA. This helps to correct dehydration, which is a consequence of excessive fluid loss. Fluids are typically given intravenously (IV) to ensure rapid absorption and effectiveness.
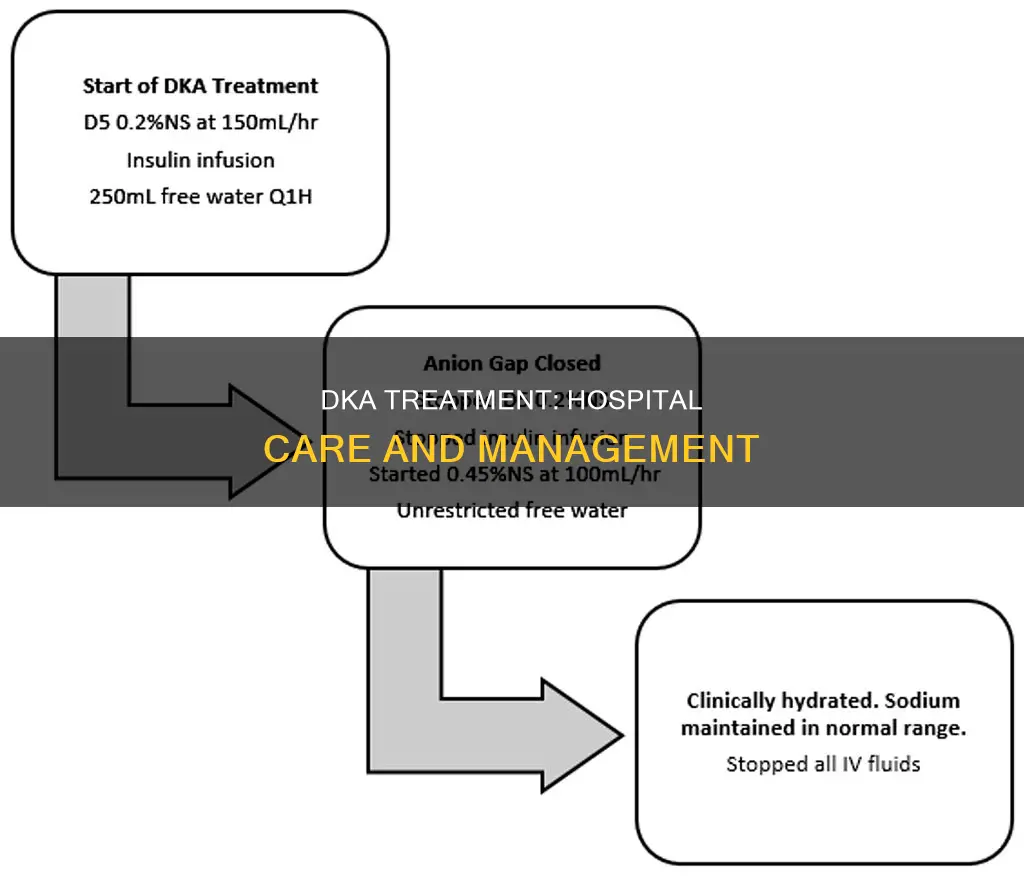
The choice of fluid for rehydration is important. Isotonic saline solutions, such as isotonic sodium chloride, are often used initially. Once the patient is stabilized, a switch to half-normal saline at a rate of 200-1000 mL/hour is recommended. This rate aims to match the fluid losses due to osmotic diuresis.
In addition to correcting dehydration, fluids also play a role in thinning out blood sugar. This is achieved by adding glucose to the hydration fluid when the blood glucose concentration reaches approximately 250 mg/dL. Typically, a 5% dextrose solution in hypotonic saline is used. This approach helps to maintain blood glucose levels within a desirable range and prevents iatrogenic hypoglycemia.
It is important to closely monitor blood glucose levels during fluid administration. Once blood sugar decreases to below 180 mg/dL, the isotonic sodium chloride solution is replaced with a 5-10% dextrose solution with half-isotonic sodium chloride. This gradual transition ensures a safe reduction in blood sugar levels.
The administration of fluids is usually followed by insulin therapy after about an hour. This timing allows for the evaluation of potassium levels, as insulin administration before adequate fluid replacement can be dangerous and less effective. Insulin plays a crucial role in reversing DKA by lowering blood sugar levels and controlling ketonemia.
Pastor TD Jakes Hospitalized: What We Know So Far
You may want to see also
Explore related products




![]()
Provide electrolyte replacement to maintain heart, muscle, and nerve cell function
Diabetic ketoacidosis (DKA) is a severe metabolic complication of diabetes, characterised by hyperglycemia, ketoacidosis, and ketonuria. It is a life-threatening condition that requires immediate treatment.
The treatment of DKA focuses on restoring the body's fluid and electrolyte balance, correcting insulin deficiency, and managing acute complications. Electrolyte replacement is a critical aspect of treating DKA, as it helps maintain heart, muscle, and nerve cell function.
Electrolytes are essential minerals in the blood, including sodium, potassium, and chloride, which carry an electric charge. These electrolytes play a vital role in various physiological processes, including nerve conduction, muscle contraction, and heart rhythm regulation. During DKA, excessive urination due to hyperglycemia leads to significant loss of electrolytes, particularly sodium, potassium, and chloride. This loss of electrolytes can have detrimental effects on the body's functions.
To replace electrolytes and maintain heart, muscle, and nerve cell function, intravenous (IV) fluids containing electrolytes are administered. The composition of these IV fluids is carefully formulated to match the specific electrolyte deficiencies present in DKA. For example, sodium chloride solutions are used to replenish sodium and chloride levels, while potassium chloride is added to restore potassium levels. The rate of IV fluid administration is carefully monitored to avoid excessive fluid overload, which could exacerbate the risk of cerebral edema.
Additionally, close monitoring of serum potassium levels is crucial, especially during insulin therapy, as insulin drives potassium into cells, potentially leading to life-threatening hypokalemia. If serum potassium levels drop below a certain threshold, potassium replacement therapy may be initiated to prevent cardiac dysrhythmias and other complications associated with hypokalemia.
DUIs: Hospital Employment Impact and Your Career
You may want to see also
![]()
Administer insulin therapy to reverse diabetic ketoacidosis
Insulin therapy is an important aspect of treating diabetic ketoacidosis (DKA). DKA is a life-threatening complication of diabetes, characterised by hyperglycemia, ketoacidosis, and ketonuria. Insulin therapy helps to reverse the effects of DKA by inhibiting ongoing lipolysis and ketone production, and promoting the regeneration of bicarbonate.
When treating DKA, it is important to closely monitor the patient and manage any concomitant processes, such as infection, cerebrovascular accident, myocardial infarction, sepsis, or deep venous thrombosis. Extreme vigilance is required during the first 24-48 hours, and intensive care is often necessary during this period.
The first hour of treatment focuses on correcting fluid and electrolyte loss. Fluids can be given by mouth or intravenously (IV). IV fluids are often used to replace fluids lost through excessive urination and to thin out blood sugar. Electrolytes, such as sodium, potassium, and chloride, are also administered intravenously to support the proper functioning of the heart, muscles, and nerve cells.
After the initial stabilisation, insulin therapy can begin. Insulin is typically administered through a vein (intravenously). Low-dose insulin is recommended, as excessive insulin dosing can be harmful. Insulin therapy should be continued until ketonemia is controlled, and blood sugar levels have dropped to about 200 mg/dL (11.1 mmol/L). A return to regular insulin therapy may be possible at this point, provided the blood is no longer acidic.
During insulin therapy, it is important to monitor potassium levels. Potassium levels typically decline as potassium reenters the intracellular compartment. If potassium levels drop too low, potassium supplements may be administered, but caution is required as low potassium levels can be dangerous.
Boston Medical Center: Top-Tier Care, Compassionate Staff
You may want to see also
![]()
Discharge patients when they can resume their daily insulin regimen
Diabetic ketoacidosis (DKA) is a serious and potentially life-threatening condition that requires urgent treatment in a hospital. It is characterized by hyperglycemia, acidosis, and ketonemia and typically occurs in patients with type 1 diabetes, although it can also develop in patients with type 2 diabetes. The treatment for DKA involves addressing fluid loss, electrolyte imbalances, and insulin therapy.
DKA patients are typically discharged from the hospital when they can resume their daily insulin regimen without a recurrence of ketosis. This indicates that their condition has stabilized and they are able to manage their diabetes effectively at home. However, it is important to closely monitor patients during their time in the hospital to ensure that they are responding well to treatment and that there are no complications.
The first 24-48 hours of treatment for DKA are critical and are typically spent in an intensive care unit. During this time, patients are closely monitored, and the focus is on correcting fluid loss and electrolyte imbalances. Insulin therapy is also initiated to lower blood sugar levels and reverse the effects of DKA.
As the patient's condition stabilizes, the medical team will work to gradually transition them back to their regular insulin regimen. This may involve adjusting their insulin dose or delivery method. The patient's blood glucose and ketone levels will be closely monitored during this transition to ensure that they are within a safe range. Additionally, the medical team will provide education and guidance to help the patient understand their DKA episode, identify risk factors, and develop a plan to prevent future occurrences.
Once the patient has met the discharge criteria, they will be released from the hospital. However, ongoing monitoring and follow-up care are crucial to ensure the patient's diabetes management remains on track and to reduce the risk of future DKA episodes. This may include regular check-ins with their diabetes care team, continued monitoring of blood glucose and ketone levels, and adjustments to their insulin regimen as needed.
Amitabh Bachchan's Role at Nanavati Hospital: Trustee or Not?
You may want to see also
Frequently asked questions
Diabetic Ketoacidosis is a serious, life-threatening condition that occurs when harmful substances called ketones build up in the blood due to a lack of insulin. It is a complication of diabetes and is most common in patients with type 1 diabetes, but it can also occur in those with type 2 diabetes.
Symptoms of DKA usually develop over 24 hours and include high blood glucose levels, arterial pH less than 7.3, and the presence of ketones in the blood or urine. Causes can include illness, injury, surgery, non-compliance with diabetes treatment, and certain infections.
Treatment for DKA in a hospital typically involves initial rehydration with fluids, electrolyte and potassium replacement, and insulin therapy. Patients are closely monitored for any complications, and treatment continues until ketone levels are safe and the patient can eat and drink normally.
With standardized treatment guidelines, the mortality rate for DKA has decreased to less than 5%. However, deaths still occur, particularly in elderly patients with other illnesses. The overall mortality rate due to hyperglycemic crisis has declined, but there is scope for further improvement, especially for certain at-risk groups.