Several factors have been found to be associated with higher in-hospital mortality. These factors include age, gender, and pre-existing medical conditions. For instance, a study on patients with aortic stenosis (AS) found that those who underwent non-cardiac surgery had a significantly higher risk of in-hospital mortality and worse outcomes. Similarly, during the COVID-19 pandemic, older patients with comorbidities such as hypertension, diabetes, and cardiovascular diseases were found to have a higher risk of in-hospital death. Furthermore, certain medical conditions like diffuse large B-cell lymphoma (DLBCL) and interstitial lung abnormalities (ILAs) have also been linked to increased in-hospital mortality rates.
| Characteristics | Values |
|---|---|
| ICU Delirium | Cardiovascular Burden and Higher Mortality in Patients with Severe COVID-19 Pneumonia |
| Age | Significantly higher in fatal cases |
| Gender | Male sex associated with an increased risk of death |
| Initial viral load | Above the cutoff of 4.45 log10 copies/mL associated with death prior to discharge |
| Aortic stenosis | Associated with higher in-hospital mortality and worse outcomes in pancreatic cancer patients |
| Cardiovascular diseases | Associated with higher in-hospital mortality in COVID-19 patients |
| Diabetes | Associated with higher in-hospital mortality in COVID-19 patients |
| Chronic kidney disease | Associated with higher in-hospital mortality in COVID-19 patients |
| Hypertension | Associated with higher in-hospital mortality in COVID-19 patients |
| Chronic respiratory conditions | Associated with higher in-hospital mortality in COVID-19 patients |
| Hospital size and specialization | No significant effect on mortality |
| Service intensity | Positive association with hospital mortality |
| Community attributes | Accounted for more variance in hospital mortality rates than organizational attributes |
| Acute kidney injury | Associated with in-hospital mortality in patients with diffuse large B-cell lymphoma |
Explore related products






What You'll Learn
- ICU delirium in patients with severe COVID-19 pneumonia
- Aortic stenosis in patients with pancreatic cancer
- Risk factors associated with in-hospital mortality during a yellow fever outbreak
- Factors affecting in-hospital mortality in patients with diffuse large B-cell lymphoma
- Hospital performance and categorisations
![]()
ICU delirium in patients with severe COVID-19 pneumonia
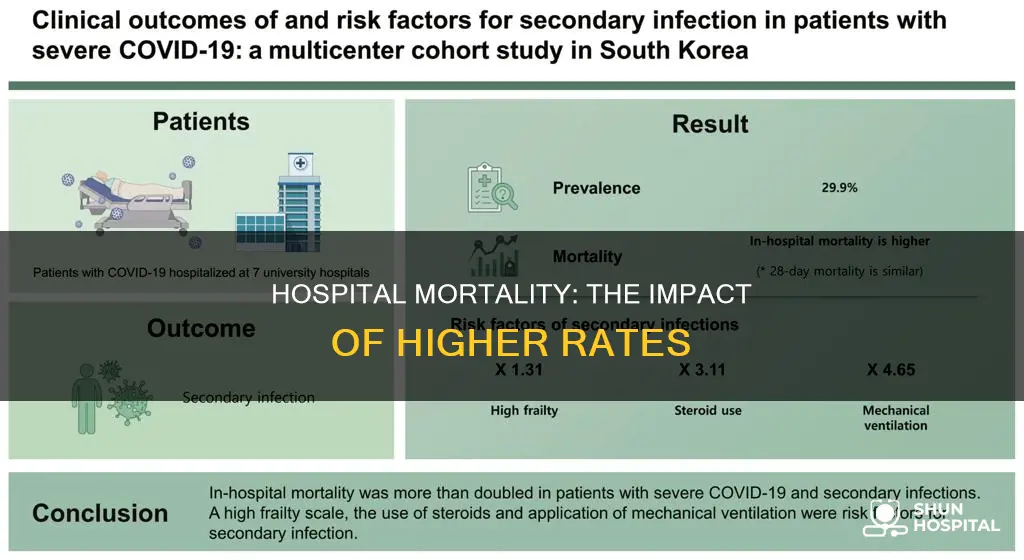
COVID-19 can lead to functional disorders and complications, including pulmonary, thromboembolic, and neurological issues. The neuro-invasive potential of SARS-CoV-2 may result in acute brain malfunction, which manifests as delirium as a symptom. Delirium is a risk factor for death among patients hospitalized due to critical illness.
A study examined 335 patients with severe COVID-19, of whom 72 (21.5%) developed delirium. The mortality rate was significantly higher in the delirium group, at 59.7% compared to 28.5% in those without delirium. Delirium increased the risk of death, with an odds ratio of 3.71. Patients with delirium were older (76.1 vs. 63.1 years), tended to be female, and were more frequently hospitalized in the HDU.
Aggressive investigation and treatment of the infection and associated systemic effects, such as hypotension, are the most effective strategies to reduce morbidity and mortality associated with delirium. The ABCDEF bundle is a management strategy that can help reduce delirium's frequency in the ICU via a synergistic approach. It includes assessing, preventing, and managing pain, spontaneous awakening and breathing trials, choice of analgesia and sedation, early mobility and exercise, and family engagement.
Delirium is a common complication of SARS-CoV-2 infection, with an incidence rate of up to 82% in ICU intubated patients. Older age and associated medical comorbidities are recognized as major risk factors for delirium development. Vitamin D deficiency is also associated with an increased risk of delirium and mortality among critically ill, elderly COVID-19 patients.
Hospitals Hiring RNs: Associate Degrees or Not?
You may want to see also
Explore related products






![]()
Aortic stenosis in patients with pancreatic cancer
Aortic stenosis (AS) is a condition that frequently coexists with cancer, as they share common risk factors. The presence of AS in cancer patients can complicate treatment options, as it increases the risks associated with oncologic surgery, cardiotoxicity, and heart failure.
A retrospective study investigated the impact of AS on in-hospital mortality in patients with pancreatic cancer undergoing pancreaticoduodenectomy (PD). Out of 16,150 pancreatic cancer patients who underwent PD, 165 (1.02%) were diagnosed with concurrent AS. The mean age of patients with AS was significantly higher than those without (74.51 years vs 66.41 years). Patients with AS had significantly higher in-hospital mortality, cardiac arrest, and intensive care unit (ICU) admissions compared to patients without AS. There was no difference in mechanical ventilation usage, hospital charges, and length of stay between the two groups.
The study concluded that AS was associated with higher in-hospital mortality and worse outcomes in pancreatic cancer patients undergoing PD. It recommended that a multidisciplinary team of surgeons, cardiologists, anesthesiologists, and physicians should jointly develop appropriate preoperative and postoperative approaches for these patients.
In elderly patients with pancreatic cancer and severe AS, the optimal treatment strategy is complex and not well established. Surgical aortic valve replacement (SAVR) is usually the standard treatment for severe AS, but it is often avoided in elderly patients with malignancy due to its invasive nature and increased perioperative risk. In such cases, transcatheter aortic valve implantation (TAVI) is increasingly performed as it may enable earlier and safer surgical intervention for malignancy.
In summary, aortic stenosis in patients with pancreatic cancer is associated with higher in-hospital mortality, particularly in those undergoing pancreaticoduodenectomy. The presence of AS complicates treatment options and worsens outcomes. A multidisciplinary approach is recommended to optimize preoperative and postoperative management for these patients.
Japan's Unique Hospital Signage: A Guide
You may want to see also
Explore related products

$8.79 $10.99





![]()
Risk factors associated with in-hospital mortality during a yellow fever outbreak
Yellow fever is a high-impact, high-threat disease with a risk of international spread, making it a potential threat to global health security. The risk of infection by sylvatic vectors in South America is highest during the rainy season (January–May), with peak incidence in February and March. The greatest risk factors associated with in-hospital mortality during a yellow fever outbreak are advanced age, male sex, and a high initial viral load.
A retrospective study conducted in Brazil during a yellow fever outbreak found that the in-hospital mortality rate was 24%. The study included 283 patients with confirmed yellow fever infection who were older than 13 years of age. The median age of the patients was 46 years, and the majority (87.6%) were male. Age was significantly higher in fatal cases, with a median age of 49.5 years compared to 46 years in non-fatal cases. Male sex was associated with an increased risk of death, with a relative risk of 4.66.
Additionally, an initial viral load above the cutoff of 4.45 log10 copies/mL was significantly associated with death prior to discharge, with an odds ratio of 12.2. Other factors that were significantly related to increased odds of death prior to discharge included log-transformed AST, INR, lactate, WBC, and age. The most common symptoms on admission were fever, myalgia, jaundice, headache, abdominal pain, vomiting, weakness, and arthralgias.
While yellow fever vaccination is generally not recommended for travel to areas with a low potential for virus exposure, it may be considered for travelers at increased risk due to prolonged travel, heavy mosquito exposure, or inability to avoid mosquito bites. The risk of acquiring yellow fever during travel can be difficult to predict due to variations in ecologic determinants of virus transmission. However, vaccination is an essential component of outbreak control, and the World Health Organization (WHO) recommends that every at-risk country has at least one national laboratory capable of performing basic yellow fever blood tests.
Epic Payment Systems: Transforming Hospital Payment Processing
You may want to see also
Explore related products






![]()
Factors affecting in-hospital mortality in patients with diffuse large B-cell lymphoma
Diffuse large B-cell lymphoma (DLBCL) is an aggressive lymphoma that arises from mature B cells. It is the most common non-Hodgkin's lymphoma and can occur de novo or through the transformation of various low-grade lymphomas. Patients with DLBCL often present with a rapidly growing symptomatic mass in nodal or extranodal tissues, such as the stomach, gastrointestinal tract, lungs, or central nervous system. They may also experience B symptoms, including fever, weight loss, and night sweats. Despite advancements in treatment, in-hospital mortality remains significant, and understanding factors contributing to mortality is crucial for improving patient outcomes.
Several factors affect in-hospital mortality in patients with DLBCL. Treatment delays in DLBCL can lead to serious complications, including sepsis, acute respiratory failure, tumor lysis syndrome, acute kidney injury, and gastrointestinal bleeding. These complications significantly impact the survival rates of patients with DLBCL.
Multivariate analysis has identified several specific events that significantly increase the odds of in-hospital mortality in DLBCL patients. These events include tumor lysis syndrome (TLS), sepsis, acute kidney injury (AKI), acute respiratory failure (ARF), and gastrointestinal bleeding (GIB). Hospitalizations with these complications are associated with longer lengths of stay and higher total hospital costs compared to those without.
Additionally, patient age is a crucial independent factor associated with DLBCL-specific mortality. The Ann Arbor stage of the disease and chemotherapy also play significant roles in predicting the prognosis of patients with DLBCL. By understanding these factors, clinicians can promptly identify high-risk patients and implement targeted clinical interventions to improve outcomes.
In conclusion, in-hospital mortality in patients with DLBCL is influenced by various factors, including treatment delays, patient age, disease stage, and specific complications such as TLS, sepsis, AKI, ARF, and GIB. Further research and understanding of these factors are essential to enhance clinical practices and improve patient outcomes in the context of DLBCL.
President's Day: Are Hospitals Open or Closed?
You may want to see also
Explore related products



![]()
Hospital performance and categorisations
Hospital performance plays a crucial role in ensuring patient safety and positive health outcomes. Several factors influence hospital performance, including the availability of resources, the competency of medical staff, and the adoption of evidence-based practices. Hospitals that excel in these areas tend to have lower mortality rates and improved patient outcomes. For instance, hospitals recognised for nursing excellence, known as Magnet hospitals, have been found to attract and retain highly skilled nurses, potentially contributing to better patient outcomes. However, it is unclear whether Magnet hospitals consistently demonstrate lower risk-adjusted mortality rates than non-Magnet hospitals.
Hospital categorisations, on the other hand, provide a framework for evaluating and comparing hospital performance. Common methods for categorising hospitals include mortality rates, patient safety indicators, and quality indicators. However, inconsistencies in hospital categorisations have been noted. In a study conducted in 2006, out of 28 hospitals with higher-than-expected mortality rates by one classification method, some were found to have lower-than-expected mortality rates when assessed using different methods. These discrepancies may arise from a lack of standardised criteria and variations in statistical methodologies.
The relationship between hospital performance and in-hospital mortality is complex and multifaceted. While certain hospitals may excel in specific areas, the overall performance is influenced by a range of factors. For instance, during the COVID-19 pandemic, factors such as limited ICU capacity, inadequate ventilation support, and a high patient-to-doctor ratio contributed to higher in-hospital mortality rates, particularly in resource-constrained settings. Additionally, patient characteristics, such as age, gender, and the presence of comorbidities, also play a significant role in determining mortality outcomes.
Furthermore, specific medical conditions and procedures are associated with higher in-hospital mortality rates. For example, patients with aortic stenosis (AS) undergoing non-cardiac surgery are at an increased risk of complications and mortality. Similarly, patients with diffuse large B-cell lymphoma (DLBCL) who experience complications such as acute renal failure, sepsis, or acute respiratory failure during hospitalisation are at a significantly higher risk of mortality. These examples highlight the importance of considering specific medical contexts when evaluating hospital performance and categorisations related to in-hospital mortality.
Chemotherapy Treatment: Hospital Stay or Outpatient Care?
You may want to see also
Frequently asked questions
A study of patients with yellow fever in Brazil found that male sex was associated with an increased risk of death. Other factors increasing the risk of death included fever, myalgia, jaundice, headache, abdominal pain, vomiting, weakness, and arthralgia.
Age, gender, and delayed treatment are some of the factors associated with in-hospital mortality among COVID-19 patients. Older patients, particularly males with chronic conditions like hypertension or chronic kidney disease, tend to have higher mortality rates. Shorter hospital stays also increase the risk of death.
Acute renal failure, sepsis, acute respiratory failure, tumor lysis syndrome, and gastrointestinal bleeding are independently associated with in-hospital mortality in patients with DLBCL. Acute kidney injury (AKI) is also a prevalent complication in DLBCL hospitalizations that result in death.
Aortic stenosis (AS) is associated with higher in-hospital mortality and worse outcomes in pancreatic cancer patients undergoing PD. Patients with AS had significantly higher rates of in-hospital mortality, cardiac arrest, and ICU admission compared to those without AS.